IRISi is a social enterprise established in 2017, providing expert advice and consultancy in the field of domestic violence, abuse and health.
They specialise in training local partners and health care
professionals to identify and refer patients affected by domestic violence and
abuse through their flagship intervention, IRIS (Identification and Referral to
Improve Safety).
They
support the local commissioning, implementation and growth of the IRIS
programme, including bid development, training for trainers, ongoing support,
national analysis and monitoring whilst also collaborating with partners to
develop innovative, evidence-based health interventions for those affected by
gender-based violence.
“Our vision is a world in which gender-based violence is consistently recognised and addressed as a health issue. Our mission is to improve the healthcare response to gender-based violence through health and specialist services working together.”
Medina Johnson, CEO IRISi
The IRIS programme has helped refer over 15,500 women to date. An IRIS programme is first commissioned within a certain geographical area.
Local IRIS teams are then recruited and trained and these teams go on to train local GPs, healthcare professionals and clinicians in recognising the signs and symptoms of Domestic Violence and Abuse (DVA) as well as how to ask the patient the right questions.
If the patient requires help, they are referred to an Advocate Educators (AE), who provides support to both the practice and the patients that are recognised and referred.
“Many of us know the statistics” says Medina Johnson, CEO at IRISi.
Medina Johnson, CEO, IRISi
“25% of women will experience Domestic Violence and Abuse (DVA) at some point in their lives. Two women are killed every week at the hands of a current or former partner, or adult family member.
Behind each statistic is a woman, a friend, a sister, a daughter, a mother, a grandmother, an auntie; most of these women will have had recent contact with health services.
How many of them will have found it difficult to say what was happening for them at home during their appointment? How many of them wanted someone to look beyond what they were saying?
How many women will have sat with a doctor or nurse who felt uncomfortable to look beyond and ask their patients about what was happening for them at home or whether they felt frightened or controlled by anyone because they didn’t think they had the right words or knowledge of the next steps to take? How many women were missed?”
“We know that DVA impacts both the mental and physical health of those it affects and that this has ramifications throughout the family.” Continues Medina. “In cold, hard business speak, we also know that DVA also costs the NHS a lot of money in terms of appointments, chronic illness and prescriptions.
Clinicians want to know how to best support patients and how to offer support. This is why they become medics. We can’t expect them to simply know what to do to support patients affected by DVA without offering training and support and onward referral pathways.
We need to support our clinical colleagues to look beyond and we need commissioners to fund this support in a sustainable way.”
The IRIS model rests on five principles:
Recognise when a patient is affected by DVA
Ask them about it
Respond in an understanding way
Refer the patient into specialist support
Make a record of the consultation and disclosure.
IRIS teams provide in-house specialist domestic violence training sessions to enable staff to become better equipped to respond to concerns and disclosures of DVA from all patients and perpetrators. Staff then receive ongoing support and DVA consultancy after training is completed from a named Advocate Educator.
Regular attendance from the Advocate Educator at team meetings helps remind staff about the service and also provides health care workers with support for any challenging cases.
If you are concerned a patient might be affected by DVA, only ask them about this if they are alone. It is not safe to ask when a patient is accompanied, even by a child.
As a minimum, have national helpline numbers to offer or the contact information for your local, specialist service. If you have safeguarding concerns then follow your usual safeguarding procedures.
Do not prescribe what the patient should do but let them know that support is available. Be sure to record the consultation in the electronic medical record. These are useful numbers for you:
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-30 14:03:482020-01-30 14:03:51Recognising Domestic Violence A Vital Requirement For Health Professionals
A Yorkshire Ambulance Service manager, who leads the Restart a Heart campaign, is heading to Sri Lanka to help improve cardiopulmonary resuscitation (CPR) training across the country.
Jason Carlyon, senior engagement lead for Yorkshire Ambulance Service based in Wakefield and project manager for the Resuscitation Council, has been asked for help by Dr Nilmini Wijesuriya of the College of Anaesthesiologists and Intensivists of Sri Lanka.
The country took part in the World Restart a Heart campaign for the first time in 2019 and more than 3,700 people were trained in CPR. Their first campaign was launched with support from Jason by phone, Skype and email and his advice and input was recognised by making him a founder member of the project.
The college is now keen to develop the campaign to make it bigger and better in 2020 and has asked Jason to spend a week in Sri Lanka to share his knowledge and experience with colleagues.
Jason will be visiting the capital city of Colombo at the end of January and will be teaching medics how to train others in CPR as well as providing advice on how to roll-out the campaign across the country.
Jason, who lives in Scarborough, said: “I am absolutely delighted to be invited to Colombo to help the college develop this important work. We have seen here in Yorkshire how successful the campaign can be and we are happy to support more people to learn this important life-saving skill with the aim of improving out-of-hospital cardiac arrest survival rates.”
Dr Wijesuriya said: “We look forward to Jason’s assistance with the development of this project, in order to raise public awareness in bystander CPR and also his expertise to make World Restart a Heart Day 2020 even more successful.”
On Restart a Heart Day 2019 in Yorkshire more than 860 volunteers provided CPR training to more than 46,000 students at 163 secondary schools across the region.
The concept of Restart a Heart Day was first developed in 2013 by the European Resuscitation Council. On 16 October 2014, Yorkshire Ambulance Service visited 49 schools and taught CPR to 11,500 youngsters – with the help of hundreds of volunteers, mostly off-duty staff and community first responders.
In 2016 Yorkshire Ambulance Service supported the roll-out of the event to all UK ambulance services and two years later it was adopted by the International Liaison Committee on Resuscitation to encourage mass CPR training on a global scale under a World Restart a Heart Day banner.
The Yorkshire event is sponsored by the Yorkshire Ambulance Service Charity and organised in partnership with the Resuscitation Council (UK), British Heart Foundation, St John Ambulance and other partners.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-29 11:01:242020-01-29 11:01:29Helping to boost the Restart a Heart campaign in Sri Lanka
Today St John Ambulance East Midlands received its first rating from the Quality Care Commission and was awarded ‘good’.
The rating comes after an inspection was announced at short notice in August last year and the CQC acknowledged improvements that have been made in the charitable service since the previous inspection in 2017.
Both the Patient Transport Service and Emergency & Urgent Care Service were reviewed, and both were found to provide safe, caring, effective and responsive care to patients.
As part of this review, the rating takes into account the regional office in Chesterfield, satellite stations at Newark and Northampton and also reviews one event in the region.
Eight ambulances were inspected across the three regions, along with twelve sets of patient records.
To finish off the in-depth review, twenty-one members of staff were spoken to, including registered paramedics, emergency care technicians, the operations coordinator, the safeguarding lead, the fleet manager, the regional accountable officer for controlled drugs, and both registered managers for the East Midlands.
The ‘well-led’ criterion was found to be ‘needing improvement’, but the announcement comes in the middle of a re-structuring period for St John Ambulance and the CQC has acknowledged further improvements in the five-month period since the inspection took place.
Feedback from the CQC reported St John Ambulance East Midlands to be safe, effective, responsive, well-lead and caring towards patients: “Staff spoke to patients with compassion and kindness, showing they respected their privacy and dignity, and took account of their individual needs.”
St John is now implementing its 2020 business strategy for ambulance provision and looks forward to welcoming the CQC back to see further improvements; not only in the East Midlands, but across the country.
St John Ambulance is exceptionally proud of the work it does, providing urgent care and support to communities across the country.
This rating proves that this work more than meets the expectations of the independent regulator of health and social care in England.
Craig Harman, the National Ambulance & Community Response Director at St John Ambulance comments: “I am pleased that the CQC found our leaders to be visible and approachable and that our people felt supported, respected and valued.’
Craig Harman, National Ambulance & Community Response Director, St John Ambulance
“I was also pleased that the inspectors witnessed good care, witnessing our people speaking to patients with compassion and kindness. Since the inspection in August we have restructured, moving to a national operational structure.’
“We will use the feedback provided by the inspection team to underpin our new national processes as we build on the hard work already carried out by our people and continuously improve the service we provide in our communities.‘
“Driving standards across the independent ambulance sector and within the event industry is a key strategic objective for St John and this CQC report is an excellent example of the work we are already doing to help us get there”.
https://ambulancetoday.co.uk/wp-content/uploads/2020/01/Ambulance_SJA_01.jpg20003008Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-24 19:43:232020-01-24 19:43:26St John Ambulance Service in East Midlands Rated ‘Good’ by CQC: First Official Rating for the First Aid Charity
By Mark Weiner, in conversation with Eli Beer (pictured) Founder & President of United Hatzalah, Published in Ambulance Today, Issue 4, Volume 13, Priceless EMS: The Volunteers At The Heart Of Prehospital Care, Winter 2019
MARK WEINER: What sort of person volunteers with United Hatzalah–do your volunteers share a common social background or professional profile? In the United States, for instance, many EMS volunteers come from families who have generations of volunteer EMS service.
ELI BEER: The amazing thing about United Hatzalah (U.H) is that everyone volunteers with us. We have volunteers from all segments of Israeli society, Jewish, Muslim, Christian, Druze, Bedouin etc.
The volunteers are doctors, nurses, bankers, lawyers, truck drivers, garbage workers, people who work in city hall; we have a Mayor, Deputy mayor, an MK, a sandwich store owner, a spice maker etc…
We do have some families with many of their members volunteering—I think the most is 6 volunteers from one family. But, in truth, all of the volunteers throughout the country feel a kinship with one another.
When they meet in any setting, professional or social, they feel an immediate sense of family even if they have never met one another before. The unity of mission really surpasses all other dividing lines. It overrides politics, religion and even nationality. The goal brings us all together.
The Jaffe family rescuers. EMT, Psychotrauma Therapist and Psychotrauma therapeutic K-9
M.W: Of course, using volunteers reduces the cost of service but does the volunteer character of U.H provide other goods that can’t be so easily quantified? For instance, are there distinctive medical benefits that a volunteer service might be able to provide better than a fully professionalized service?
E.B: Yes, in the field of EMS it is greatly beneficial to have volunteers in addition to paid personnel. The volunteers add so much with their spirit. The extra passion and motivation which they bring to the profession helps motivate the paid staffers as well.
In Israel, we have incredible EMS personnel who work in the eld for a living but if it wasn’t for volunteers rushing out to emergencies and supporting their efforts, their own motivation would be much lower.
We all know that the paycheques for EMS work aren’t that lucrative but having volunteers around who support the work of the paid staff is crucial for raising the level of motivation across the board.
When I see services that don’t have a volunteer component, there is a much larger danger of paid first responders getting worn out, especially as the salaries are as low as they are.
In terms of benefits in a medical sense, the fact that we have people coming from other fields and joining the EMS profession as a volunteer means that they have a high level of drive and desire to help.
They bring a wealth of knowledge and experience from their own eld to emergency medicine and that knowledge juxtaposing with the knowledge of emergency medicine leads to a lot of innovation in the operational sphere, both on the macro and micro-level.
We’ve had two major projects emanate from this type of hybrid innovation. The first began with an EMT who is a therapist.
She noticed that the people witnessing a medical emergency often suffer from shock and emotional stress and need treatment in addition to the patient who suffered the emergency.
She created a specialized unit of therapists, psychologists, and psychiatrists who are tasked with responding in the eld to medical emergencies where someone is suffering a severe emotional or psychological stress reaction.
This early intervention has been shown to prevent the onset of ASR, ASD and hopefully prevents PTSD from developing. This unit is called the Psychotrauma and Crisis Response Unit and is a unique innovation of our organization.
Members of the Psychotrauma and Crisis Response Unit in Jerusalem
Another project which came from responder innovation in the field is our Ten Kavod (Giving Honor) project, where trained EMTs visit elderly people who live alone once a week.
The Ten Kavod project aims to prevent older people who live alone from feeling abandoned by society and passing away without anyone noticing.
Having a trained EMT visit them once a week provides a much-needed social outlet as well as monitoring their medical status on a regular basis. The program is run in partnership with social services on a city-wide or community-based level.
M.W: How about benefits for the individual volunteers? Does volunteering with U.H increase the civic standing of volunteers within their communities?
E.B: United Hatzalah cares very deeply for its volunteers. An integral part of our organization is making sure the volunteers feel connected to each other and to the organization.
We do this by dividing the country into 75 regional chapters based on geography and make-up of each area.
These chapters are responsible for holding social and educational meet-ups for the volunteers every six weeks, and twice a year they must have an event geared towards the families of the volunteers.
Each volunteer receives annual gifts for their families, providing the families of the volunteers with a sense of connectedness to the organization. Without the family supporting the volunteer’s work, the volunteer would not be able to drop everything at a moment’s notice and rush out to save lives.
Psychotrauma and Crisis Response Unit team members provide psychological and emotional stabilization following building fire in Jerusalem along side medical first responders
Additionally, the Psychotrauma and Crisis Response Unit contact each of the volunteers after a medical emergency that is considered to be traumatic for the responders.
The unit is tasked with checking in with the volunteer and ascertaining that they are okay from a mental health perspective following the incident.
With regards to the community itself, our volunteers are respected by their community and people look to them when they have emergencies.
This doesn’t necessarily give them a higher standing in the community but it helps the community as a whole become more resilient by knowing that, when there is an emergency, there is a person in the community whom they can turn to for help.
M.W: So, there are quite a few ways in which you believe a community benefits from having EMS provided by volunteers. Do you think that the decentralized organizational structure of United Hatzalah contributes to these benefits?
E.B: Yes. The fact that the organization is run by volunteers who come from the community means they are in touch with the needs of that community and are more concerned with patient care than a government service whose primary concern is paying the bills and thereby strongly recommends ambulance transport for any and all incidents.
A United Hatzalah beach rescue
Such a system not only overloads the hospital ERs but doesn’t always have patient care as its top priority. When EMS is a business and dependent on the bottom line of financial solvency in order to function, patient care can sometimes take a backseat to the need to transport a patient.
When service is always free of charge to the patient, nothing takes away from the high level of patient care offered by the provider. As everything in United Hatzalah is provided to the patient free of charge and done by a volunteer, the patient’s well-being is the sole motive for treatment.
M.W: Is there a distinctively Jewish ethical justification for EMS volunteerism? United Hatzalah provides services to all people, regardless of their religion, and its volunteers come from diverse religious backgrounds. But is there a way of thinking about volunteering as an EMT from the perspective of the Jewish tradition?
E.B: I think that there is a Jewish ethos of volunteering to help others in less fortunate situations across the board. Israel, as well as Jewish communities in the diaspora, has a plethora of volunteer organizations that deal with almost every aspect of life.
From free loan societies to helping with automotive troubles on the road, to EMS, to a volunteer police force—the Jewish people have always placed high importance on helping others, especially members of their own community.
There are plenty of references to this in the Bible, as well as Rabbinic literature, but I believe that the main reason for this is our unique history. We were a people apart who were, for 2,000 years, strangers in other lands.
We needed to help each other in order to survive and there has always been an understanding that no one from our community can make it on their own, so we need to band together to make it together.
United Hatzalah fleet of ambucycles
I believe that this ideology has translated into a national and individual subconscious need to help others. Our forefather Abraham was known for his acts of loving kindness.
His examples are told to all of our children throughout the ages as actions to exemplify.
M.W: Finally, Eli, is there something that other nations can learn from the historical experience of Israel about the social and cultural importance of emergency medical volunteerism or public emergency medical training?
E.B: I think that our message has resonated across the globe. When I spoke at the Ted Med event in 2013 I was asked by people from countries all over the world to come and explain our model so that they could copy it.
We have been working with other cities in many places to develop a model of our volunteer network in a way that works for them; usually in a style that is non-threatening to existing response systems and working with, rather than against, the current system.
Currently, we have active chapters in five other countries and we are always looking to expand into other cities and other countries to help save as many lives as possible.
It is my dream that no one should ever die because they were waiting for help to arrive.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-20 01:12:382020-01-20 01:12:40United in Benevolence: An Interview with Eli Beer, Founder & President of United Hatzalah of Israel
By Mark Weiner, in conversation with Magnus Andersson Hagiwara, Ph.D (pictured) of the Centre for Prehospital Research at the University of Borås, Published in Ambulance Today, Issue 4, Volume 13, Priceless EMS: The Volunteers At The Heart Of Prehospital Care, Winter 2019
Magnus Andersson Hagiwara, Ph.D., is Associate Professor at PreHospen, the Center for Prehospital Research, in the Department of Caring Science, Work Life and Social Welfare at the University of Borås, Sweden.
MARK WEINER: What role do volunteers hold within Swedish EMS? Are there any volunteers within either the re or ambulance services?
MAGNUS ANDERSSON HAGIWARA: In EMS there are no volunteers in Sweden. When it comes to the fire department the question is trickier. There are three levels of fire personnel: 1) fire fighters working full time. They live at the re station during work; 2) part-time fire fighters who have other ordinary work but are on call one week at time. They need to be at the fire station within five minutes after the call. They have the same responsibilities as the full-time fire fighters; and 3) standby fire fighters. These fire fighters have an emergency alert at home and it is voluntarily for them to respond to a call or not. They are paid only when they respond to a call. I suppose you can call the last category volunteers.
I think that EMS workers in Sweden are not seen as heroes. They are just workers doing what they are paid for. Personnel in the fire brigade have a higher status
M.W: Turning specifically to the ambulance service, how many years of training are required of personnel before they ride in an ambulance? Could you describe what it takes to become a Swedish EMT?
M.A.H: In the past, ambulance care was executed by EMTs with a short education in prehospital care (20–40weeks), but since 2005 all ambulances are staffed by at least one Registered Nurse (RN) with medical responsibility, in accordance with Swedish law. EMTs need have a three-year high school education and then a 40-week EMT education.
RNs have three years’ additional education leading to a bachelor’s degree. A specialist nurse in prehospital emergency care has one year of additional training.
Swedish ambulance nurses in a training exercise
An ambulance team in Sweden includes an EMT along with an RN, a prehospital emergency care nurse, or an RN with another specialist education such as anaesthesia or intensive care. The RN independently administers around 30 different drugs according to written guidelines and general delegation.
The proportion of RNs in Swedish prehospital care has been estimated at 68–78%. The proportion of RNs with specialist education varies widely between regions from 20 to 85%.
M.W: Do ambulance services have a civic presence in their communities beyond their immediate role of responding to emergencies and treating patients?
M.A.H: Sadly no. I think that most of the EMS workers in Sweden want to have a greater civic presence. Today, it is the fire brigade which does this kind of work. They have CPR courses in the streets. They talk about risks at home and so on.
Many EMS workers feel that they are better prepared to do this. But the reason they don’t is organizational. All ambulances in Sweden are hosted by a hospital and they are not willing to pay for this kind of activity. The fire brigades have a national organization (MSB) which sees this kind of activity as a part of the mission.
M.W: Could you describe the general cultural perception of Swedish ambulance personnel and EMS more generally? Do they tend to be seen more as heroes or as simply another class of professional doing a job?
A Swedish ambulance nurse on standby
M.A.H: I think that EMS workers in Sweden are not seen as heroes. They are just workers doing what they are paid for. Personnel in the fire brigade have a higher status and are more “heroes.” The reason is that they have taken that role and have been successful in promoting their important role in society. Fire brigade have a government agency (MSB) which controls their operations, while EMS is controlled by their respective area hospitals.
M.W: Sweden has long been renowned for the great deference that people give to elite experts—it’s the land of social engineering, after all. How might you describe the lack of a volunteer tradition in the medical field (as opposed to, for instance, local sports clubs, in which Swedes are avid volunteers) as an outgrowth of this aspect of modern Swedish society? Do you think this is positive or negative?
M.A.H: Sweden is a country with a high social protection network where we pay high taxes for health care, school and other social services to function. I think we have for a long time become accustomed to the state taking care of this for us.
Another reason may be that we have not been at war for the last 150 years. For example, if you compare with Finland who was severely affected during World War II, the Finnish people have a completely different approach to civil defense.
In the summer of 2018, we had severe forest fires in Sweden. Then people realized that the state may not be so reliable after all. After that summer, there has been a big increase for various volunteer groups who can move out and help in crises.
I myself was extinguishing fires in northern Sweden then and was impressed with how civil society took over when the state failed.
https://ambulancetoday.co.uk/wp-content/uploads/2020/01/Weiner-speaking-with-a-Swedish-ambulance-nurse.jpg30244032Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-19 23:28:452020-01-19 23:28:49Voluntarily Independent: An Interview with Magnus Hagiwara, Ph.D.
By Mark Weiner, in conversation with Dr.med. Joachim Schiefer, MSc. (pictured) of the Austrian Mountain Rescue Services, Published in Ambulance Today, Issue 4, Volume 13, Priceless EMS: The Volunteers At The Heart Of Prehospital Care, Winter 2019
Dr.med. Joachim Schiefer, MSc., is a specialist in trauma and orthopedic surgery and sports medicine with Praxisgesund in Tamsweg, Austria. He is senior physician and head of medical training for the mountain rescue service in the region of Salzburg.
MARK WEINER: What role do volunteers play in the Austrian mountain rescue service? About what percentage of the ground-level personnel are volunteers? Do those volunteers have training in wilderness emergency medicine?
JOACHIM SCHIEFER: The Austrian mountain rescue is nearly 100% voluntary, there are only some administraton workers in the offices who are paid. In Salzburg for example, there are 3 persons for the main office and 1415 volunteers in 44 local organizations. All volunteers get a free training in all aspects of wilderness rescue.
That starts after a trial year with a three-day medicine course, followed by a weeklong winter course, and weeklong summer course, and ends with a glacier course.
All courses have medical parts with theory and practice, for example in the winter course we teach avalanche rescue and hypothermia in theory and praxis. After four years of learning and passing all exams you get a Bergretter.
Austria is a mountain region and all kinds of sports are done there. Being a Bergretter is a great honor and lots of people are interested in their exciting work.
M.W: Is there a role for volunteers in the Austrian urban ambulance corps?
J.S: There is a clear role for both terrestrial mountain rescue and urban rescue. Some volunteers do both and therefore are double educated. Some also work in hospitals and do rescuing in their free time.
The helicopter services are separate and also are staffed with people from the Bergrettung. If you work for them you get paid and also get paid for course lessons.
M.W: What type of person joins the mountain rescue service? Are volunteers drawn from the communities in which they live? How do you recruit and retain them?
Manouvering the patient uphill
J.S: Usually they come from the communities they live, so it is possible to fulfill their commitments in the region they know well.
Normally they are young mountaineers when they start the work in the rescue.
There is a strong fellowship in the organizations and lots of climbing and ski mountaineering is done together. The recruitment is organized by the local organization and if the new members do well in the trial year they start with the courses.
M.W: Are Austrians generally, and patients in particular, aware that the service is significantly based on volunteers? How do you promote awareness that it is?
J.S: The Austrians know that this is based on volunteers and lots of companies support mountain rescue, so the volunteers can leave their working place for rescuing or get free holidays for courses and teaching, especially military or police.
Working with avalanche probes, volunteer rescuers from SDMA can find victims who have been buried in snow
There are also some efforts by the Austrian government to get volunteers one week’s extra vacation or an early old age pension.
M.W: How important is the mountain rescue service to the civic life of the community? Does it host events to which the public are invited? And does being a mountain rescue volunteer confer community respect and what one might call “social capital”?
J.S: Absolutely, a lot of events are hosted by the mountain rescue, for example training for the local community, or work in avalanche commissions. The communities have an obligation to the organization to give them space for their vehicles and a social room for their meetings.
M.W: Since 2009 the television show “Bergretter” has been a popular television series. Could you reflect on the importance of the show or on other representations of the mountain rescue service in popular culture?
J.S:As mountaineering gets more popular every year people also get more interested, especially in the rescuing part. Austria is a mountain region and all kinds of sports are done there. Being a Bergretter is a great honor and lots of people are interested in their exciting work.
M.W: Are there reasons for the mountain rescue service to substantially involve volunteers in addition to cost savings?
SDMA cliff face extraction
J.S: Yes, a lot of money is saved for the Austrian state. Mountain rescue is traditionally a non-profit organization, it always was voluntary. With the money paid for the rescues and also the sponsoring of companies and national and local communities we can offer teaching on a high level and acquire all the equipment for the local organizations.
It would be much more expensive for the whole of Austria if everyone would be paid. Being a member of mountain rescue is of high prestige in my country. Mountain equipment is cheaper for us if we buy it; we receive preference in job applications; etc.
M.W: What role does the mountain rescue service play in providing local communities a sense of self-governance?
J.S: The mountain rescue is guided by the central organization of the districts (for example Salzburg or Innsbruck); administration and education is organized there and equal for all.
Transporting the patient across the deep snow
This guarantees the same standards for the whole country. There are meetings in Salzburg where everyone comes together to discuss and renew. Every voice is important. For the local community, it is very important to have their own rescue service.
Mountainous Austria has a lot of remote areas, so there are lots of local specialties. As I noted before, for a little town in the mountains it brings prestige to have its own mountain rescue service.
The Austrian Mountain Rescue Services (SDMA) employ 12,500 rescuers all of whom are volunteers. Whilst Federal Law in Austria dictates that costs must be paid by the person who was rescued, SDMA have somehow managed to work out an insurance policy of just €28 per year for global coverage in mountain rescue which also covers all family members, life partners and children under 18 living in one household. This covers patients for up to €25,000 with a one week rescue operation easily costing around €20,000. At the time of writing, in 2019 SDMA has saved 641 people and undertaken 703 rescue operations.
https://ambulancetoday.co.uk/wp-content/uploads/2020/01/An-SDMA-rescue-dog-helps-volunteers-in-the-search-for-a-patient-1.jpg8501280Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-19 21:48:352020-01-24 20:19:37High Prestige: Volunteers in the Mountaintops
By Mark Weiner, in conversation with Capt. Dale Drescher (pictured) of the Virginia Beach Volunteer Rescue Squad, Published in Ambulance Today, Issue 4, Volume 13, Priceless EMS: The Volunteers At The Heart Of Prehospital Care, Winter 2019
A retired school teacher, Dale Drescher is Captain of Administration and member of the Executive Committee of the Virginia Beach Volunteer Rescue Squad in Virginia Beach, Virginia, USA. She has been a member of the City of Virginia Beach Emergency Medical Services, and VBVRS, since May 2013.
MARK WEINER: Are there reasons for community EMS organizations to be based on volunteers, or to have a significant volunteer component, other than the cost savings they provide?
DALE DRESCHER: It’s a matter of community pride. We have a saying that we actually print on the side of my squad’s ambulances: “neighbors serving neighbors.”
There’s been a general buy-in here to the idea that community health involves being a part of something larger than yourself. We want to show that we are a community willing to give time and energy to something that we feel is important for the health of our city.
Also, Virginia Beach is a very large resort area. We get about 2.8 million visitors a year, particularly in the summertime. They are often surprised and very pleased when we have to treat and transport to find that they’re not going to get a bill.
We have a very large military contingent, because of the naval and joint forces bases located in our area
I’ve had occasions when a person has said to me, “you all helped my family the first time we ever came on vacation three years ago—and we like it here in part because of that feeling.” We hope that the spirit of VBVRS actually draws visitors to our area.
We give people an opportunity to put a foot in the medical eld as they look toward some kind of medical career. The way we structure volunteering, it’s 48 hours a month required duty time. If we were a paid service they likely wouldn’t be able to gain that kind of experience.
M.W: Is it important to you that residents appreciate you’re a volunteer organization? How do you promote that understanding?
D.D: It is very important to us. We want the community to know. But it’s also a bit of an uphill battle for us. In general, people associate first responders with fire and police and those are traditionally paid services.
If we have a patient in our ambulance and they’re in a comfortable situation and want to talk, we always tell them that this is a free treatment transport, that we’re volunteers and we do not charge for service. It’s word of mouth.
We always participate in any PSA opportunity, particularly during EMS week; local radio stations and the TV stations will offer us the ability to come on and talk about what we do.
We have a rescue foundation for all 10 squads whose mandate is promoting volunteerism. The rescue foundation does a lot of recruitment. Its website is vbrescuefoundation.org.
Two Virginia Beach Rescue crews standing strong
M.W: What kind of people volunteer for the service? Do they tend to have a similar background, or are they from different walks of life?
D.D: It’s very interesting. It’s sort of across the board. There’s a large portion of the demographic that is young, and that makes sense when you think that they are starting out and they are looking to the future and thinking, ‘is a medical career something that I’m interested in’?
We allow people to begin serving with us at age 18, so we have a good portion of people who are in college and we work with those people to allow them to remain active volunteers if they’re at a school outside of our 35-mile range. We really work hard to keep that demographic part of us.
We have a lot of people who volunteer in their 30s, 40s, and 50s. They want to do something outside the home and the family—people who work full time and still manage to volunteer on the weekends.
Everything in your training is taken care of financially—and in return you sign a contract to give the city of Virginia Beach one year of service. The cost for the city is about $3000.
And then we have a very large military contingent, because of the naval and joint forces bases located in our area.
I had someone recently join our squad and she came from a base in San Diego. She said she chose this area as her next duty station because we were a volunteer-based organization. She looked all over the country to find that.
And finally, we have people in the 50-plus range who are looking toward retirement. They want to start thinking of something beyond the working years.
We also have a small portion of people who change careers in midstream. I have someone in my squad right now, who is an orthopedic surgeon; he retired and became an EMT. I have someone else who is an attorney by trade but has decided to go back to medical school.
The Virginia Beach Volunteer Rescue Squad Advanced Life Support Unit, as featured at the 2018 EMS World Expo
M.W: Do you have any volunteers who come from a family tradition of EMS volunteerism?
D.D: Many of them. All ten squads have families with multi-generational members. It is common in my squad because the volunteer system in our city started down near the ocean front area and that’s where we’re located. I very frequently have college students come to volunteer and say, “Oh, my mom and dad both worked here.”
We also have couples that met and married there. I can think of at least three who are active now. They became volunteers and they met at the squad.
One couple consists of the husband, who is in the military, while she’s a stay-at-home mom. When they hand off the baby, one comes off duty and the other one goes on—and the baby is in the carrier!
M.W: Do you have any challenges with recruitment and retention, and how do you address them?
D.D: Traditionally I think the city has seen sort of ups and downs in recruitment and they seem to follow the pattern of employment. If there’s a period of really full employment in the country, our recruitment tends to go down a little bit.
If we have a period of time where there are people who can’t find jobs, then they look to volunteer opportunities. But in the last five or six years, we have had really large classes in our EMS Academy.
The Virginia Beach Volunteer Rescue Squad Advanced Life Support Unit, as featured at the 2018 EMS World Expo
The city has a wonderful program which makes it easier for us to recruit: they pay for the schooling in our academy. You get all of your training for free. Textbooks, lecture time, operational scenario training, practical exams, all of that comes through the class.
When a student passes the class, the Academy is certified to administer the Virginia practical exam, which the student does not pay for; and EMS pays for the student to take the NREMT exam.
Everything in your training is taken care of financially—and in return you sign a contract to give the city of Virginia Beach one year of service. The cost for the city is about $3000.
The city has a wonderful yearly awards program. Each year we have a call-of- the-year award. And we have many scholarship opportunities.
If you come on board and you’re interested in taking the science classes you need to be able to apply to PA school or become a paramedic, then you can apply for a scholarship.
M.W: What’s the public perception of EMS and EMTs in Virginia?
D.D: When we have people who come and settle here they generally expect that whoever is an EMT is part of the re service. That’s common across the country and they are taken aback at times that we have an absolutely separate, standalone EMS system in the city of Virginia Beach.
Drescher and partner Roy White at the station
If we have an EMS call and we have both a re crew and an EMS crew and we’re all in different uniforms, there’s a little bit of confusion as to why we’re all there and looking a little different from one another.
But once they realize that re does an initial assessment if on scene first, and then EMS takes over, they don’t seem to feel that there’s anything negative attached to that separation.
In general, it’s been my experience that the people that I treat in transport feel that the EMTs are knowledgeable. They seem to trust us. We seldom get any really negative response.
M.W: What about the social status of EMTs? Is it high?
D.D: Probably down a step below fire and police because people are more familiar with them. People know police, they see them as heroic in certain circumstances, and I think they certainly do with fire.
With EMS, I don’t think they have the visual. We don’t carry guns, and we’re not running into burning buildings. In terms of public perception, maybe we’re viewed as maybe a step down in terms of heroism.
Founded by attorney Peter J. Holland III in on May 1st 1952 the Virginia Beach Rescue Squad serves roughly 1,000 volunteers serve 440,000 residents (plus tourists) as part of the City of Virginia Beach EMS Department, offering patients a completely free emergency service.
Acknowledging the voluntary aspects of this vital EMS service to the city, the Virginia Beach Rescue Squad Foundation was created in 1982 by Bernard M. Stanton, in order to give financial support to what are now the 10 rescue squads that make up the City of Virginia Beach EMS Department across the city’s 225 square miles, each squad being a non-profit organization in its own right, relying entirely upon fundraising (and also saving the US taxpayer around 22 million USD per year).
https://ambulancetoday.co.uk/wp-content/uploads/2020/01/vb-rescue-2.jpg5501920Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-19 19:57:222020-01-19 20:57:38Community Calling: An Interview with Capt. Dale Drescher of the Virginia Beach Volunteer Rescue Squad
By Mark S. Weiner Published in Ambulance Today, Issue 4, Volume 13, Priceless EMS: The Volunteers At The Heart Of Prehospital Care, Winter 2019
Let’s engage in a thought experiment about EMS financing. Imagine a perfect world for every accountant tasked with balancing the books of every ambulance service across the world. EMS coffers are veritably over owing with money from direct government support, lavish insurance payouts, and philanthropic giving. Each month, the accountants saunter into meetings with formerly despondent service chiefs, spread open their red-lined ledgers, and smile broadly. “Spend away,” they announce in joyous unison. “Spend like there’s no tomorrow!”
In this what-if world, every ambulance station has multiple top-of-the-line service vehicles, the most innovative ALS equipment, and a helicopter or two. In every common room, free donuts pop out of silver dispensers at the push of a button. EMT uniforms are stitched with gold thread. Finally, and most important—at least for this issue of Ambulance Today—unlimited resources make it possible to staff all ambulances entirely with full-time, well-paid professionals. No volunteers.
Would this “ideal” world of fully professionalized emergency medical services be desirable? Or would it erode essential qualities of EMS that we should take care to value, preserve, and enhance?
When volunteers offer their services for free and pledge to serve all patients no matter what their background or condition, they help define their community as bound by ties of underlying humanity rather than in terms of commerce or hierarchical power.
I believe that it would, and that appreciating why can also help us further grasp the role of EMS in a democratic society—the subject of this series of occasional essays.
Let’s consider three justifications for EMS volunteerism and how they might fare in the ideal world of our thought experiment.
The most common reason given for volunteerism is easy to understand, and it’s a good one: it reduces costs.
In many parts of the world today the only feasible way to deliver ambulance services is for some providers to work for free. Even in the first world, cash- strapped rural and suburban counties sometimes face a similar challenge, notably in the United States, with its tradition of local public service financing (for a recent discussion, see the NBC news story “What if you call 911 and nobody comes?”).
We might call this the justification of institutional necessity.
While it’s compelling on the surface, this justification isn’t especially deep. Most important, it doesn’t provide a reason for volunteering that can’t be overridden in flush financial times. In the world of unlimited resources described above, it would provide no reason to use volunteers at all.
What’s worse, the logic of institutional necessity can easily be twisted to justify professional inequity or even exploitation. Just ask any underpaid EMT working today in a for-pro t service. “Sorry, Jack, sorry Jane, we can’t pay you what you’re worth: we just can’t afford it. But thanks for showing up.”
Few organizations reject free labor, especially if it’s provided by well-trained men and women willing to throw themselves into stressful situations and put their own health at risk.
In other words, beware of making necessity a virtue!
Working with avalanche probes, volunteer rescuers from SDMA can find victims who have been buried in snow (article linked to interview with SDMA as part of this series)
So, we might turn to a second justification: EMS volunteerism is commonly hailed for providing volunteers with special career benefits. Volunteering as an EMT is an excellent way for young people to explore the medical field and decide whether a career in medicine is right for them.
It also looks great on a medical school application. Speak with just about any ambulance service that uses volunteers and you’re likely to encounter this worthy line of argument.
Call it the individual justification.
The individual justification is the mirror image of the institutional justification: from its perspective, the benefits of a volunteer system ow not to the ambulance service as an institution but rather to service members.
A host of related arguments fall under this umbrella. For instance, some people assert that volunteering should be encouraged because it offers volunteers a chance to feel pride in contributing to the common good, motivated solely by their values—surely a positive thing.
Yet these justifications don’t provide a reason for volunteering that’s intrinsic to the nature of EMS.
If students think they might be interested in pursuing a career in medicine but wonder whether it’s truly a good fit, it’s of course helpful for them to be able to offer free labor on board an ambulance, but it’s by no means necessary. They could volunteer at a local hospital, or shadow physicians on their rounds.
Similarly, people who wish to reap the personal benefits of volunteering can seek out any number of other volunteer opportunities. Why volunteer for EMS as opposed to a soup kitchen? Or the telephone company? Both provide valuable public goods that one could feel good about delivering.
The individual justification isn’t wrong. It’s simply limited.
Most notably, except in cases when EMS as an institution is inextricable from the individual good sought—for instance, when volunteering helps young people decide whether they would like to pursue a career specifically in ambulance work—the justification wouldn’t carry much weight in a world of unlimited resources.
Should an ambulance service go through the trouble of recruiting, retaining, and managing volunteers simply so that a small group of individuals can advance careers outside of EMS or fulfill their personal sense of ethics—which they also could do in any number of other ways?
Armed only with the individual justification, leaders of EMS organizations balancing the costs and benefits of volunteers would surely opt for institutional efficiency: staffing ambulances solely with full-time professionals.
An SDMA rescue dog helps volunteers in the search for a patient (article linked to interview with SDMA as part of this series)
Finally, there’s a third type of justification, one that’s neither institutional nor individual. Instead, it is social. It justifies the use of volunteers within EMS because they advance the common good by fostering public health.
At first glance, this common-good-as- public-health justification might seem the most unassailable of the three. Surely any practice that advances the public health should be encouraged!
But to see why this argument for EMS volunteerism would likewise fall in our what-if world, we can ask ourselves a question: What public health goods do EMS volunteers advance distinct from those which EMS can supply without them?
Obviously, EMS provides enormous benefits to individuals and society.
But to argue that the use of volunteers in EMS should be supported because volunteers advance the individual and collective interests that EMS can meet without volunteers is essentially to raise the institutional justification: volunteering is good because EMS is good and volunteers can effectively help EMS fulfill its mission.
This is true, and it’s a worthy view, but it wouldn’t get us far in our thought experiment.
There is, however, a variation on the social justification that fares much better: the civic justification.
The civic justification argues that EMS volunteerism benefits the common good defined as the political life of a community—using the broadest sense of the term political.
In making this argument, this justification posits that the public benefits of EMS volunteerism are at once (1) separate from the primary goods provided by the ambulance service, because they can be provided best, or perhaps only, through the use of volunteers; and (2) unique to EMS, or nearly unique, because they are intimately connected to the character of emergency medical services as a social practice.
Put another way: the civic justification suggests that volunteers in EMS provide important public benefits that can’t be provided by paid professionals, and that something about the nature of EMS makes it especially well suited to provide those goods.
What public benefit does EMS volunteerism advance, unique to EMS, other than the public health? In a phrase: it contributes in unique ways to the culture of democratic solidarity.
United Hatzallah rescue boat on the Sea of Galilee (article linked to UH Interview as part of this series)
To appreciate why, we need to add another term into our discussion: civil society.
Civil society consists of those myriad social institutions that are distinct from government, the family, and the marketplace. Religious organizations, sports clubs, social reform movements, political advocacy groups—these institutions lie at the heart of liberal democratic life.
They are sometimes said to “mediate” between the family, an institution devoted to highly particular interests, and the state, which is devoted to the universal interests of the public as a whole.
Healthy democratic societies are like a vegetable soup chock-full of such institutions—they come in every flavor. Yet their magic lies in how, in their very diversity of interests, they contribute to social cohesion.
They do so by creating ties of affection between their members as they pursue common ends, while also encouraging them to understand their activities in broad community terms.
Indeed, historians and sociologists tell us, civil society institutions also ultimately tend to foster a common national identity—an essential value for democratic societies seeking to accomplish collective goals.
EMS volunteer groups are civil society institutions in all the usual, classic respects. They are neither the family (families call EMS precisely when they are no longer capable of assisting one of their members), nor are they agents of the state.
They lie midway along the continuum of particularity and universality. They bring people together in pursuit of common interests. They contribute to social solidarity in the same ways that most other civil society institutions do.
Yet volunteering for EMS is different from contributing labor to other civil society organizations, even ones dedicated to fully public-regarding ideals. There is something about EMS that makes the way it contributes to social solidarity unique and essential.
What is it?
In my first article for this series, I described the siren of an ambulance as having both an instrumental value—to clear the road—and, less appreciated, a cultural value: it’s a signal that the most basic duty of the state is being fulfilled. Volunteers within EMS serve a related cultural signalling function.
Virginia Beach Volunteer Rescue Squad at the 2019 Veterans Day Parade (article linked to interview with Virginia Beach Volunteer Rescue Squad as part of this series)
Most importantly, when EMS volunteers are identified as volunteers, they signal to the people they serve that their community is characterized by a spirit of mutual interdependence and popular sovereignty.
By appearing on scene, they announce that their patients live in a world in which people literally take care of each other, down to the core of their physical being, and in which residents are active participants in governing themselves.
In the language of contemporary social criticism, volunteers convey an empowering, even liberating vision of “bio-politics”—a way of organizing society that fosters independent, self-sufficient community self-care.
This cultural signalling can be undertaken best, and perhaps only, through the work of volunteers. The lack of financial compensation within volunteer EMS organizations differentiates them from both the marketplace and the state.
When volunteers offer their services for free and pledge to serve all patients no matter what their background or condition, they help define their community as bound by ties of underlying humanity rather than in terms of commerce or hierarchical power.
EMS is uniquely well-suited as a field to provide this cultural signal because of the nature of its core work: safeguarding individual life in emergency situations.
EMS can be contrasted in this respect with the military, the police, and the re service, all three of which are also central to a well-functioning society, involve significant personal sacrifice, and are closely associated with EMS by ties of friendship. Unlike the military, for instance, EMS is devoted entirely to saving life, never to taking it.
In addition, the military is directed outward, toward securing the territorial integrity of a country, rather than inward, as is EMS (when a country’s military force is directed inward, to quash a domestic insurrection, the foundations of the society are rocked).
VA Beach Volunteer Rescue Squad Unit 1425, a 2018 Ford Horton model (article linked to interview with Virginia Beach Volunteer Rescue Squad as part of this series)
EMS personnel also differ fundamentally from their brothers and sisters in the police force, even while they may rely upon one another in the field.
Most importantly, EMS is non-normative and non-coercive: we don’t judge our patients, we don’t carry guns, and we generally won’t transport people against their will. When police respond to an emergency, someone is likely to face the consequences of having done something criminally wrong.
EMS most resembles the fire service, which is likewise devoted to non-normative, non-coercive, ameliorative activity. Yet there is a subtle but important difference between the two groups.
As a public service, fighting fires is justified in large part because one burning building poses a threat to other buildings around it. It wasn’t long ago that a burning building could set an entire town ablaze.
The social justification for the ambulance service is much less communal. Patients receive treatment almost entirely because they are viewed as morally worthy of care in themselves.
Nobody is concerned that unless a medic attends to Jim’s basilar skull fracture it will spread to Janet. EMS is dedicated to saving individual life, in other words, without regard to whether a patient’s chief complaint implicates the community at large.
A United Hatzalah beach rescue (article linked to UH Interview as part of this series)
These characteristics make volunteer ambulance services especially potent signals of civic solidarity. In providing life-saving care to individuals simply as human beings, and in taking up the responsibility of doing so personally, they communicate the cultural ideals that make healthy democratic societies work.
It’s for this reason that they are worthy objects of community pride: they lie at the heart of what community means in the first place.
In turn, volunteer EMS programs suggest that as civil society institutions, they would be justified even in the financially flush times of our thought experiment.
They would be justified not simply because they lower institutional costs, enable individuals to explore their careers and fulfill their ethical obligations, and foster public health—all of which are worthy goods—but also, at their core, because they are culturally irreplaceable and essential.
A final thought. Across the world today, liberal democratic societies are being driven by an anti-elite politics that collectively goes under the name of populism.
These politics take different forms in different places, and readers of this magazine will naturally have many contrasting views about populist political movements and the individuals who lead them, both for and against.
But there is one aspect of all such movements upon which everyone can agree: They are driven by a feeling and a rhetoric of existential threat.
In advanced industrial democracies, most notably, a significant portion of the electorate has come to understand that it has been politically abandoned.
United Hatzalah fleet of ambucycles (article linked to UH Interview as part of this series)
Its members fear that, in an underlying, implicit, often unspoken way, they are dying, or at the risk of it, both as individuals and communities, and they resent that the establishment has turned its back on them.
What we have witnessed on the world stage in recent years are the political consequences of a massive breakdown of social solidarity.
The causes need not concern us here—they are well outside the scope of EMS. But the remedies should, because at least one of them does lie within our scope.
Whenever an ambulance shows up at a door—especially when the man or woman stepping from the vehicle provides their services for free—it announces that society has yet to fracture into a million little pieces under the pressures of market competition; that people are still motivated by love and community as much as by personal profit; and that strangers will give their time and risk their health and, in the deployment of their skills, tell a suffering fellow citizen, in essence: “You are not forgotten. We will take care of you. Your community is here.”
This is not to say that EMS should add the repair of social bonds in a fractured world to its mission.
It is to say that it is something we do already, both as volunteers and as full-time professionals, and that it therefore would be worth our time to think about this aspect of our work more carefully and systematically than we already do. Doing so might help us inform our practice and support our advocacy.
The four interviews accompanying this essay are meant to contribute to this conversation. They ask questions of EMS representatives in four countries with different volunteer traditions, providing a spectrum of opinion and experience—and food for thought.
Interview #1 with Capt. Dale Drescher of the Virginia Beach Volunteer Rescue Squad Interview #2 with Dr. Joachim Schiefer of the Austrian Mountain Rescue Services (SDMA) Interview #3 with Eli Beer, Founder & President of Israel’s United Hatzalah Interview #4 with Magnus Andersson Hagiwara, Ph.D. from the Centre for Prehospital Research at Sweden’s University of Borås
In a forthcoming article for this series, I will consider a subject intimately related to this one: the cultural status of EMS and its representation in popular media. If you have thoughts about the issue, I hope you will reach out to me via email or social media.
Mark S. Weiner, J.D., Ph.D., EMT-B,
volunteers for the Seymour
Ambulance Association in
Connecticut, USA. He is the author of
The Rule of the Clan: What an Ancient
Form of Social Organization Reveals
about the Future of Individual Freedom
(Farrar, Straus and Giroux, 2013),
winner of the Grawemeyer Award for
Ideas Improving World Order.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-19 18:35:572020-01-20 01:22:58EMS for Democracy: Ambulance Volunteers as Cultural Agents of Solidarity
A
father of four has thanked South Western Ambulance Service NHS Foundation Trust
(SWASFT) after he survived a cardiac arrest.
Kevin
Scott, 40, collapsed and stopped breathing while looking after his children at
home in Westbury, Wiltshire.
The
children raised the alarm, and family friends did CPR and used a community
defibrillator to resuscitate him.
Paramedics
provided further treatment, and transported him to hospital. He went on to make
a fantastic recovery.
The
family made a special trip to Trowbridge Ambulance Station on Sunday 5 January
to thank staff personally.
Kevin
said: “Thank you to everyone who helped to save my life.
“I
have no recollection of what happened, but I have been told of the wonderful
care the paramedics and hospial staff provided.
“Without
the actions of our children, our friends, the paramedics, and the availability
of the community defibrillator, things could have turned out very differently.”
Katrina,
Kevin’s partner, said: “This was the worst imaginable experience for our
family, but the response could not have been better. Thank you to everyone for all
you did. You are all heroes!”
Kevin has a rare condition called situs inversus totalis, which means his heart and other organs are on the opposite site of his body to normal.
From left to right: SWASFT Operations Officer Michael Anning, Kevin Scott, his partner Katrina Cherry, and their children Jayden, Aiyana, Elysia and Leyton.
His
sudden cardiac arrest happened in the kitchen in front of his 10-year-old daughter
Aiyana in April 2019. His 13-year-old daughter Elysia got help, and his 15-year-old
son Leyton called 999 to inform SWASFT.
999
Call Handler Georgia Birch instructed those on scene who were providing basic
life support, while other control room staff organised for crews to be sent to
the scene.
Georgia
told those on scene to get the nearby defibrillator, which Elysia ran to get.
The
family friends, who were doing CPR, used the defibrillator to give Kevin two
shocks to restart his heart.
SWASFT
Operations Officer Michael Anning arrived first on scene to find Kevin
breathing for himself. Michael was soon followed by specialist paramedics
Daniel Tucker and James Hubbard. They were also joined by ambulance crew Alice
Holt and Angela Welch.
The
team stabilised Kevin at the scene and transported him to hospital in Bath
before he was transferred to Bristol.
Kevin
was fitted with an implantable cardioverter defibrillator (ICD) in an effort to
prevent it happening again.
Michael
said: “The patient’s children were extremely brave in gaining help quickly and
obtaining the defibrillator. The lifesaving interventions, including the bystander
CPR, made all the difference to Kevin.
“It
was great to meet the patient and his family on behalf of the entire ambulance
team, including the call handler who provided crucial instructions before we
arrived.”
If you suspect someone is having a heart attack or cardiac arrest: call 999 immediately, begin CPR, and use a public access defibrillator if one is available.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-19 15:24:382020-01-19 15:24:42Family Thank Ambulance Service After Dad Stops Breathing
By Joseph Heneghan, Editor, Ambulance Today, Published in Ambulance Today, Issue 3, Volume 13, Ahead of the Curve, Education and Technology Special, Autumn 2019
At first glance, WoundClot looks like nothing particularly new. The gauze material visually holds so much in similarity to other haemostatic gauzes, you could be forgiven for completely overlooking what is actually a truly massive step forward in emergency trauma care.
In reality, this new and revolutionary gauze has four main groundbreaking features going for it.
Firstly, it holds up to 2,500% of its own weight in blood and is actively absorbent for up to 24 hours.
Secondly, WoundClot has a truly remarkable wound surface adhesion. The pliant 3D gel matrix adheres to surrounding tissues in the wound and will not be dislodged by patient movement, wound manipulation, or high-pressure bleeding, while remaining easy to remove without causing rebleeding.
WoundClot’s third attribute is the ability to create an environment that is conducive to clotting by concentrating platelets, red blood cells and clotting factors in its 3D gel matrix.
This leads to a clotting ability which has, so far, left any individuals working in trauma care or surgical theatres unanimously stunned.
The spurting from the carotid artery was stopped within just 15 seconds.Each first responder and ER physician involved in the case was, as you would imagine,completely stunned at how quickly the bleeding had been controlled.
The gauze is also effective on patients that are undergoing anticoagulant therapy or, in the case of severe traumatic injuries, patients that are coagulopathic, utilising multiple mechanisms of action to achieve haemostasis. For the more scientifically minded of you, WoundClot is made from cellulose, a natural fibre product found in plants.
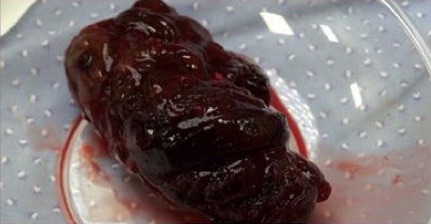
WoundClot® gauze converting to gel
It is the onlyNon-Oxidised, Non-Regenerated Cellulose Structure (NONRCS) productin the world, meaning that it possesses the highest safety profile of any haemostatic gauze available, whilst requiring little to no triaging to use effectively.
A further testament to its truly remarkable and game-changing nature, WoundClot is also notably small. It achieves all this in 8x20cm, 8x100cm, and 20x30cm sizes (CE Class IIB). The longest measurement there is just over three feet.
I should mention that other sizes are available for the Class III Surgical Implant version of the product too, they have covered all bases here. The Class III product comes in 5x10cm and 10x10cm and, very importantly, has the fastest bioabsorbability profiles around today.
Finally, and by far its most notable revolutionising aspect, is that it is applied without compression. Whether it’s for catastrophic bleeding, for haemorrhaging, or for arterial spurting, you don’tapply pressure to it.
To be perfectly honest, I am quite convinced that adopting this new and revolutionary product is not just a logical obligation, but an ethical must.
You place the gauze on the site of the wound, lightly press around it so that the fabric comes into contact with the blood, and then you take your hands off and leave it well alone, leaving you free to attend to anything else that demands your immediate attention.
As you can imagine, this is especially useful in patients with multiple injuries, or in Multiple Casualty Incidents, where a single provider would be otherwise engaged in holding pressure for at least 3-5 minutes with other haemostatic products.
Two minutes post-application
There have been many examples of the proficiency of WoundClot of late, which show just how revolutionary this product is, how vital it is to have in any kit, and which have often left professionals both in prehospital and hospital settings simply stunned.
Again, this is a world-wide, first-of-its-kind development. It may look like a run-of-the-mill gauze, but it isn’t.
One such recent story is indeed a sad one, as one of the victims of the case sadly passed after being transported to hospital. And it is her that this detail focuses on.
Recently in Pittsburgh a case occurred where an armed attacker stabbed two women, seemingly at random, at a downtown bus shelter. One escaped with a non-fatal wound to the mouth. Harrowing and traumatic for her none-the-less, but she survived.
The first victim, however, was much more unfortunate. As a police officer was speaking to her, to genuinely check on her welfare as he had seen her sleeping or possibly passed out in said bus stop, the attacker sprung from behind him and stabbed the poor lady directly in her carotid artery.
As quickly as he could, the officer detained the attacker to prevent any further stabbings beyond the two which had just occurred and then swiftly ran back to the first woman, placing his finger within the wound to try to stem some of the arterial spurting. The police noted that medics arrived quickly on scene1.
At around the same period, a representative of WoundClot had been in Pittsburgh training police staff on the application of the gauze, as the local P.D. had recently adopted it as part of their standard kit. Whilst riding with members of their SWAT team, she attended this call.
Six minutes post-application
Finding an off-duty paramedic attending, and understandably struggling to control the arterial spurting, they offered a simple 3×39 inch piece of gauze (just a little over 3 feet long).
The spurting from the carotid artery was stopped within just 15 seconds. Each first responder and ER physician involved in the case was, as you would imagine, completely stunned at how quickly the bleeding had been controlled.
It is a terrible thing that this poor woman never made it. But the applications of this revolutionary advancement in haemostatic gauze cannot, and must not, be overlooked or ignored.
Here, it was clearly a matter of time. Not speaking as a medic, but purely as a member of the public with a basic education and common sense, anyone can tell you that the chances of survival from a punctured or severed carotid artery are amazingly slim, and they get even slimmer as every second passes.
But it’s clear to see that if this product, compact and easily carried by any first responder—police, fire, or EMS—were adopted as a vital part of every emergency kit, then application could be employed much quicker.
8 minutes post-application
I would personally go a step further and say that these should be made readily available on the street in the same way that AED’s are. That they should be given out to older children in schools with a very simple and easy to follow demonstration on how they should be applied.
As professionals in prehospital emergency care, each one of you know that traumatic bleeding can occur from a seemingly endless possible array of injuries and accidents at any time: as the result of a harrowing attack such as the one outlined above, as the result of a child running into a glass plate, as the result of a saw slipping on a construction site.
What if this product was as common as a household band-aid? What if its amazingly simple application, which any adult or child could reasonably follow (taking into consideration factors such as panic, fright and trauma of course), was just as widely known?
How many catastrophic lacerations could be controlled within minutes or less? How many lives could be saved? What if you could turn up to a call where the patient’s traumatic bleeding is already under control, allowing you to focus on stabilising, or resuscitating, and then transporting?
According to the US Army Institute of Surgical Research (ISR), 84% of potentially survivable injuries ended in fatality due to uncontrollable haemorrhage. Of these, 67% of the injuries did not allow for sufficient access to the traumatic wound for the attending medics to be able to either place compression or fix a tourniquet2.
And now, at long last, we finally have a haemostatic gauze which requires no compression. The first, and only one, of its kind.
WoundClot® Gauze post-clotting
To be perfectly honest, I am quite convinced that adopting this new and revolutionary product is not just a logical obligation, but an ethical must.
However, the proof is in the application. It’s totally understandable that it is mentally difficult to move on from current accepted practices and to accept when a totally new and revolutionary product arrives, trusting in something you have never used before when so much is at stake.
When you have controlled so many traumatic bleeds, knowing that constant and firm compression is vitally important, it can be very hard for you visualise some miracle gauze which allows you simply place it over the bleed without compression, whilst you watch it firmly bond to the wound all of its own as it begins to absorb the bleeding and create a successful clot.
That’s why Ambulance Today can proudly offer free samples to any organisation which is forward thinking enough to see how vital this is to their deployment of life-saving emergency care.
And it is undoubtedly vital to every organisation within this field.
If this is something you have control of then I advise you to get in touch with us. If not, then I advise you to take this article to your supervisor and to advise them to get in touch with us.
You have nothing to lose, and the patient, and their families, have everything to gain. It’s free. If you find that we’re wrong, then you simply continue with whatever it is that you’re currently using. However, we remain highly confident that this won’t be the case.
Dr Shani Eliyahu-Gross.“Non-Compression Applications for Arterial Hemorrhage Control With WoundClot Hemostatic Gauze”. http://www.woundclot.com/wp-content/uploads/2016/06/Non-Compression-Applications-for-Arterial-Hemorrhage-Control- with-WoundClot-Hemostatic-Gauze.pdf
https://ambulancetoday.co.uk/wp-content/uploads/2020/01/Screen-Shot-2019-09-08-at-03.12.13.png220911Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-01-14 15:46:522020-06-27 12:23:44A World First: A Completely New Development in Haemostatic Gauze Promises Massive Success in Traumatic Bleeding and Haemorrhage Control
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, you cannot refuse them without impacting how our site functions. You can block or delete them by changing your browser settings and force blocking all cookies on this website.
Google Analytics Cookies
These cookies collect information that is used either in aggregate form to help us understand how our website is being used or how effective our marketing campaigns are, or to help us customize our website and application for you in order to enhance your experience.
If you do not want that we track your visist to our site you can disable tracking in your browser here:
Other external services
We also use different external services like Google Webfonts, Google Maps and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.