Two staff from the Welsh Ambulance Service that came to the aid of a young man who presented himself to them with severe lacerations have been recognised with a CEO’s Commendation.
In a presentation at Cardiff East Ambulance Station on Monday 2 March, the story of how Non-Emergency Patient Transport crew Nick Boswell and Alex Adams, from Cardiff, went over and above the call of duty was told.
The pair had pulled up at Newport Road traffic lights in November of last year, on their way to a routine non-emergency patient when they were flagged down by a young man in a frantic state.
Alex immediately put the hazard warning lights on and Nick, who was in the back of the vehicle, opened the doors to be greeted by another man clearly severely wounded and entering into a state of shock.
Nick, who also has 10 years St John Ambulance experience, recalls the victim’s friend shouting “He’s been stabbed, he’s going to die”.
“I checked for signs of an assailant first and got the victim on board as soon as I could and shut the doors” said Nick.
Left to right: David Thomas, Nick Boswell, Jason Killens and Alex Adams
“He had three visible injuries but was bleeding heavily from an arterial wound which he had wrapped his own t-shirt around it as a makeshift bandage.
“I applied a blast dressing to the wound and elevated his arm in an attempt to stem the bleeding” he continued.
Meanwhile in the cab of the ambulance, quick thinking colleague Alex, remained calm and made the vital calls.
He said: “I radioed control to notify emergency medical colleagues and also called 999 for assistance from my mobile.’
“I stayed on the line providing updates on the patient’s condition and location details.”
All the while, Nick and Alex kept talking to the young victim to keep him calm and conscious.
The pair’s Operational Team Leader, David Thomas, was soon on scene and helped Nick apply another dressing to the wound which was still bleeding heavily.
Upon arrival of the emergency ambulance, and by now the police, the crew were able to move from the busy city centre traffic to a nearby bus stop and, after applying a tourniquet to the victims arm, transferred him to the emergency ambulance and on to the University Hospital of Wales for treatment.
David said: “Once the patient had been handed over I had a good chat with both members of the crew to make sure they were alright.’
“We then had to wait for the police CSI team to complete their investigations.”
Alex was able to take the vehicle back to their station where it was locked up before being taken away for deep cleaning.
The pair had a thorough debrief with David and were also referred to the service’s Trauma Risk Management team for mental welfare checks after such a traumatic and unexpected event.
Alex said: “We had marvellous support from all of our colleagues at the station plus chats with senior staff and offers of counselling.”
Remaining humble and playing down their actions that day, Nick said: “We are trained in First Aid and basic life support, but when people see an ambulance vehicle, they expect help. That’s all we did.”
Alex who is just 24 years old said: “It was a bit overwhelming.’
“But in the moment, you just do what you need to do.”
Welsh Ambulance Services NHS Trust Chief Executive, Jason Killens, made the presentation and said of the pair: “Nick and Alex exemplify true healthcare professionals.’
“They were faced with an unexpected and highly traumatic situation but remained calm, applying their training and experience, to help aid a positive outcome for the patient.’
“As a service, we are extremely proud of them for their actions that day, actions that saved a young man’s life.’
“It was fantastic to meet them and extend our gratitude and respect.”
At the ceremony, Alex was watched by his proud father Dave Adams who has 35 years’ service with Welsh Ambulance.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-08 13:49:582020-03-16 21:10:33Staff Recognition for Aiding Young Victim
North East Ambulance Service (NEAS) dispatch supervisor has won a national Control Room Award for going above and beyond the call of duty.
Dispatch supervisor for unscheduled care, Martin Lonsdale was nominated by his colleagues after he saved a passenger from a burning car.
He was shortlisted out of three others and won in the category for special recognition for bravery and courage.
As a dispatch supervisor, Martin is at the central core of the Trust, sending emergency ambulances to patients.
As a former Royal Marine, serving in Afghanistan and recently becoming a qualified volunteer community first responder to life-threating emergencies; he has the essential instinct to save lives.
Martin Lonsdale
Whilst driving on his way into work for his shift at NEAS headquarters, he came across an over turned car in the road. He ran over to find three people in the car, one of which was trapped in the rear seats.
Martin said, “When I was inside the vehicle trying to get the person out, within minutes, flames engulfed the front of the car.’
“People around me were shouting to get out of the way as it looked dangerous. But I just couldn’t go without attempting to save the passengers life.’
“My instinct was purely to help save those people.’
Martin proudly displays his Unsung Hero Control Room badge
“I managed to get the seatbelt undone but the patient fell on top of me, trapping me in the confined space inside the car.’
“I had a moment where I genuinely thought I was going to die alongside the patient. I thought of my family and that’s when I managed to find the strength to get the patient out of the car.
“Many others were helping me and the person to get to safety and after we got a few yards away from the vehicle, it exploded, taking everything with it. Had we been any longer in the car, it would have been a very different story.”
Assistant dispatch service manager Andy Bell has worked with Martin for many years and wanted to recognise his heroic efforts by nominating him for the control room award.
Jury’s Inn Hinckley Island, Hinckley, Leicestershire, United Kingdom, 02 March, 2020. Pictured, left to right: Matthew Griffiths, Martin Lonsdale, Helen Fospero. Award: Bravery and Courage Sponsor: UK Cloud Presenter: Matthew Griffiths Winner: Martin Lonsdale Organisation:Maritime and Coastguard Agency Control Room Awards 2020
Andy said, “Martin’s actions didn’t surprise me; he showed the upmost gallantry and valour in a life-threatening situation.’
“He always tries his best and shows great integrity with everything that he does. His family would have been at the front of his thoughts throughout the whole incident.’
“Even though the situation meant Martin risked his own life, we were relieved to hear that he left the scene unscathed. Fortunately, everyone escaped unharmed thanks to his heroic actions.’
“I am so proud of Martin — he is an inspiration to us all.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-07 22:24:272020-03-09 11:12:06North East Ambulance Service Control Room Supervisor Awarded for Heroic Efforts
The charity supports the pioneering service to deliver life-saving treatment to the 10 million people who live and work in London, bringing the hospital to the scene to deliver urgent medical care when every second counts.
In 2019, the charity’s 30th anniversary year, the helicopter and rapid response cars took an advanced trauma doctor and paramedic to 1,730 patients whose lives were on the line.
The figures show 74 more missions than the previous year, at a cost of £2,080* to make each mission happen.
Primarily funded by charitable donations, the service is also supported by Barts Health NHS Trust and the London Ambulance Service NHS Trust.
Barts Health NHS Trust provides the doctors, some financial support and the helipad facilities at the Royal London Hospital and London Ambulance Service NHS Trust provides the paramedics and the emergency infrastructure to dispatch the service 24 hours a day.
The data shows that the busiest boroughs were Westminster, Haringey and Lambeth.
Nearly one third of injuries were from stabbings and shootings (32%) or road traffic incidents (28%) and one fifth due to falls from height (22%).
Other critically ill patients were treated following rail incidents, industrial accidents, drownings and medical emergencies including cardiac arrest.
London’s Air Ambulance has a world class reputation for delivering clinical innovation and pioneering treatment at the roadside and is known for using new technology and treatments to bring the most innovative care to the people of London.
Treatments now delivered by the team on-scene include pre-hospital REBOA to help patients suffering serious internal pelvic bleeding, and carrying blood on board.
These treatments have resulted in a significant drop in number of patients bleeding to death before reaching hospital.
In 2019, London’s Air Ambulance started working with ‘GoodSAM instant on scene’ — a technology that enables London Ambulance Service Paramedics working within dispatch to live stream video from any 999 caller’s mobile phone camera.
This allows then to get on-scene video footage, instantly locate the caller, and provide life-saving advice. It has been used by the service 134 times since October 2019 and has been a great help in quickly understanding a patients’ injuries, ensuring London’s Air Ambulance is dispatched to the right person in the quickest time.
Jonathan Jenkins, CEO of London’s Air Ambulance Charity, said: “Every day, London’s Air Ambulance is ready to deliver rapid response and cutting-edge medical care to people who are in urgent need, but we couldn’t do it without the support of the public.’
“Every second counts in an emergency — we hope the public will continue to help us get there in time to save a life by donating at www.londonsairambulance.org.uk.”
Medical Director Dr Tom Hurst said: “Critical injury from road traffic incidents, falls from height, assaults and other injuries are the biggest killer of people aged under 40.’
“We have a proud history of pioneering new ways to save lives and have developed ground-breaking treatments that mean people who would have died at the scene of the incident a few years ago are now surviving.’
“Sadly, there are still some patients whose injuries are so severe that they don’t survive. That’s why we are committed to investing in research and development and collaborating with our partners to find new techniques and treatments that can create more survivors in the future.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-07 21:46:512020-03-16 17:40:41London’s Air Ambulance Charity Calls for Support to Fund Growing Number of Missions
By Audrey Fraizer, Managing Editor, Journal of Emergency Dispatch Published in Ambulance Today, Spring 2020, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
Lynne Baird believes her son Daniel would have survived had he been treated with a bleed control kit.
Daniel was 26 when fatally stabbed at a pub in Digbeth, Birmingham, following a night out with friends and, to prevent others from suffering the same fate, Lynn started a foundation distributing bleed kits in London’s financial district.1
Baird’s
precautionary contribution is not isolated.
Taxi Alliance Liverpool received training in bleeding control and bleeding control kits from the Aintree University Hospital’s trauma centre as part of a KnifeSavers campaign.
The kits contain scissors, gloves, tourniquets and trauma dressings as well as military-grade gauze and chest wound sealant.2
KnifeSavers
was the brainchild of Nikhil Misra, consultant general and trauma surgeon at
Aintree University Hospital, who wanted to make tools that could prevent death
closer to the scene.
“Equipping people with the knowledge and tools to prevent massive blood loss at the scene of a stabbing is the single most effective step we can take towards improving the chances of survival for victims.”3
Knife crime has reached a new record high in England and Wales, with official figures revealing almost 44,700 offences in 2019.4 UK Office of National Statistics show that the City of London saw a steep rise in knife crime last year, up 43 percent to 57 incidents in 2018-19.5
A fifth of the crimes – more than 4,500 – were committed by children aged between 10 and 17.6
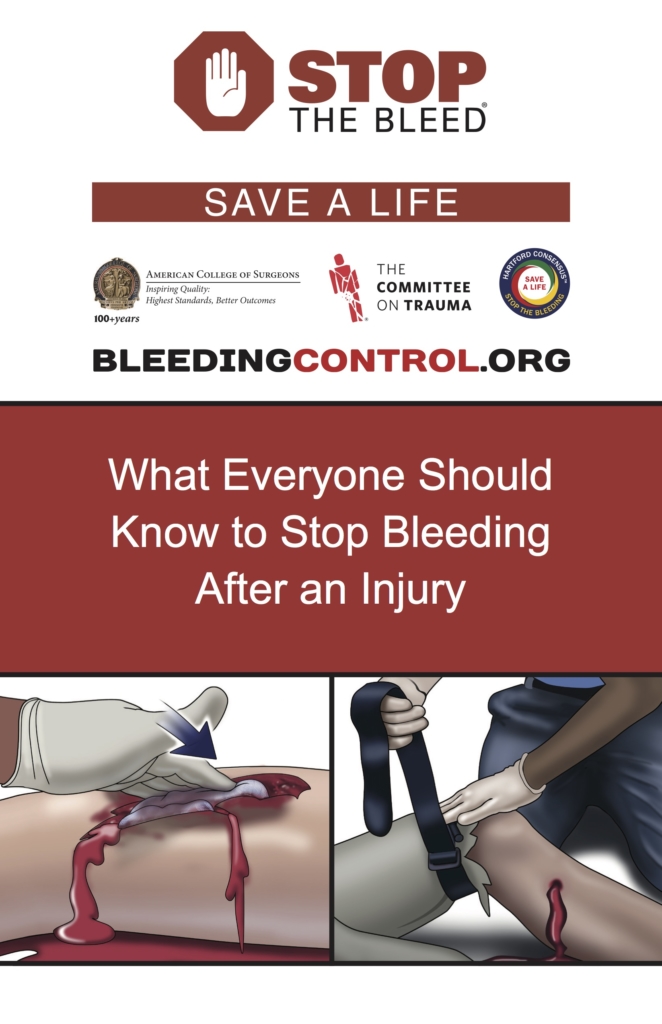
Would you know how to help someone with major bleeding? Uncontrolled, life threatening hemorrhaging is one of the leading causes of preventable death following a traumatic injury, and a person who is bleeding uncontrollably can die from blood loss within five minutes.
1st Lt. Rob Fidler, 19 Regiment Royal Artillery Joint Tactical Air Controller of cer-in-command, applies a tourniquet to a simulated injury on Master Sgt. Scott Piper, 352nd Special Operations Support Squadron Medical Element ight chief. U.S. Air Force members had conducted two-day training with British JTACS from 19 Regiment from Tidworth, Wiltshire, and 3 Battalions. (U.S. Air Force photo by Karen Abeyasekere)
Think
tourniquet. They’re back in EMS vogue as a device in hemorrhage control
following a decline of the tourniquet in favor of applied pressure during WWI.
Medical tourniquets now play an essential role in complex medical procedures and emergencies to regulate blood flow.
These devices are used to prevent blood loss by compressing blood vessels and assist medical professionals in carrying out medical procedures with minimum blood loss.
Tourniquets are not limited to a one-style fits all description but come in several varieties to accommodate the purpose.
They include tactical, pediatric, military, surgical, and the emergency medical tourniquet.
An emergency medical tourniquet is commonly used to control arterial blood flow.
Numerous studies supporting the tourniquet’s return has the device counted among the essential gear of re/EMS systems and stationed alongside AEDs at airports, popular nightlife venues, and places of potential mass casualty incidents.
The International Academies of Emergency Dispatch (IAEDTM) is a charter member of the US ‘Stop the Bleed’ campaign and instructions for tourniquet use are available in the Medical Priority Dispatch SystemTM (MPDS) system version 13.2.
Protocol T: Tourniquet was developed by an Academy research team that spent the better part of a year drafting the proposal and pre-testing prior to a volunteer focused study conducted at selected venues in Salt Lake County, Utah (USA), and enlisting 246 volunteers.
Photo courtesy of Emma Hammett, First Aid for Life
The objective was determining whether layperson callers can effectively stop simulated bleeding using an improvised or a commercial tourniquet, when provided with scripted instructions via phone from a trained protocol-aided EMD.
According to the study rationale, if tourniquets are going to be placed in public locations, emergency medical dispatchers (EMDs) should be prepared to answer callers’ questions regarding situations requiring them, and enthusiastically provide instructions on their use.6
At each study sight, participants called a simulated 911 line (comparable to the UK 999 three-digit emergency exchange) and reported a victim with life-threating bleeding to the leg, which is identified in the real world as7:
• Blood that
is spurting out of the wound
• Blood that
won’t stop coming out of the wound
• Blood that
is pooling on the ground
• Clothing
that is soaked with blood
• Bandages
that are soaked with blood
• Loss of all
or part of an arm or leg
The emergency
dispatcher verified the catastrophic nature of the bleed and proceeded in
giving the step-by-step instructions while a research team member timed how
long it took the “caller” to stop the bleeding with the tourniquet, according
to the control device.
“We could
watch how people reacted [in response to the instructions] but we couldn’t step
in,” said Chris Olola, Ph.D., Director, Biomedical Informatics and Research,
IAED. “It took a lot of testing and revision before adding it to the existing protocol.”
According to results, a majority of participants (80.49%) were well within the critical five-minute time limit, with an overall median time for all trials (i.e., elapsed time from the start to the end of the simulation) of 3 minutes and 19 seconds.8
Image Credit — stopthebleed.org
“Of course,
in a chaotic, uncontrolled, and emotionally charged real-world event (such as a
knife stabbing) it might be unrealistic to expect the high success rate of
patient survival that was demonstrated here”, Olola said.
“Nevertheless,’
he said, “This study provides ample evidence that life-saving tourniquet
application by untrained laypersons is possible with the bene t of
dispatch-directed EMD assistance.”
The Tourniquet protocol doesn’t replace direct pressure in most bleeding situations, cautioned Greg Scott, Operations Research Analyst, IAED.
“A tourniquet is the best way to stop the bleeding from catastrophic injury. Direct pressure is still the preferred method for abrasion.”
As in the EMD’s First Law of Safety, the bystander is cautioned against creating “more victims at the scene.”
Bystanders must ensure their own safety and provide care to the injured person if the scene is safe to do so.
If safety is threatened, the bystander should move from the danger, taking the victim if possible, to find a safe location.
Not surprisingly, demand for surgical tourniquets has surged based on their reintroduction to trauma care and the rising adoption rate of trauma care devices, along with increasing numbers of accidents, injuries, and emergencies.
Additionally, the range of new devices being developed offer promise for bystanders, first responders, and surgeons delivering emergency services and these devices are expected to play crucial roles in reducing the emergency response times and improving the survival rates for patients.9
References
1 Wright M. “Pubs and clubs in London’s nancial district to be given stab kits.” 2019; Nov. 19. https://www.telegraph.co.uk/news/2019/11/18/ pubs-clubs-londons-financial-district-given-stab- kits/ (accessed Feb. 10, 2020). 2 Hughes L. “Five minutes is all it takes to bleed to death but this kit could change that.” Liverpool News. 2019; Oct. 21. https://www.liverpoolecho.co.uk/news/liverpool-news/five-minutes-takes-bleed-death-17117547 (accessed Feb. 10, 2020). 3 See note 2. 4 Dearden L. “Knife crimes reach record high as prosecutions fall to record low.” The Independent. 2020; Jan. 23. https://www.independent.co.uk/ news/uk/crime/knife-crime-uk-stabbing-ons-police-england-wales-prosecutions-a9298166.html (accessed Feb. 10, 2020). 5 See note 1. 5 See note 4. 6 Scott G, Olola C, Gardett M, et al. “Ability of Layperson Callers to Apply a Tourniquet Following Protocol-Based Instructions from an Emergency Medical Dispatcher.” 2020; Jan. 21. Prehospital Emergency Care. http://mc.manuscriptcentral.com/pec (accessed Feb. 10, 2020). 7 Pons PT, Jacobs L. “Save a life: What everyone should know to stop bleeding after an injury.” Chicago, IL: American College of Surgeons. 2016. https://www.bleedingcontrol.org/resources/how-to-stop-the-bleed (accessed Feb. 10, 2020). 8 See note 6. 9 “Surgical Tourniquets – Creating a “Bloodless” Field of Vision for Surgeons.” Future Market Insights. 2 Aug.; 2019. https://www. futuremarketinsights.com/reports/surgical-tourniquets-market (accessed Feb. 10, 2020).
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-06 12:34:562020-03-06 13:21:14Return of the Tourniquet: Vital Tools Placed Closer to Scene
From: Cowley A, Durham M, Aldred D, Crabb R, Crouch P, Heywood A, McBride A, Williams J, Lyon R. (2019) ‘Presence of a pre-hospital enhanced care team reduces on scene time and improves triage compliance for stab trauma’. Scan J Trauma Res Emerg Med 27(86).
By Alan Cowley, Criritical Care Paramedic, SECAmb Published in Ambulance Today, Spring 2020, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
Penetrating trauma is on the rise, everywhere (Allen et al., 2019). Once the preserve of the hardened inner-city paramedic, it has crept out to every service in every area and can just as easily happen in the quaint village down the road, as the deserted back street behind a run-down metropolitan tower block.
Penetrating trauma is sly. It catches us at our most vulnerable; in the early hours of the night, swamping us with stimuli – darkness, flashing lights, crowds, adrenalised bystanders and patients, police, rearms units.
We hear the well-known mantra of penetrating trauma in our heads, “5 minutes and leave, 5 minutes and leave”, but a big part of us just wants to disregard that and for it all to be fine.
The patient ‘seems’ ok, the wound ‘looks’ ok, can I see the wound base?
Bearing in mind it has taken me 5 minutes to write this, is it really fair to expect ambulance staff to take control of this situation so quickly, bearing in mind the infrequency with which it is encountered (Henderson et al., 2019)?
In reality, what is the length of time we are spending on scene?
Figure 1: Total knife crime in England & wales (excludes Greater Manchester) [Allen et al. 2019]
These are questions we wanted to answer when starting our study (Cowley et al., 2019). As a group of specialist paramedics, we felt ‘anecdotally’ that when we arrived at scene, there was a general apathy towards scene times.
So, we looked into it. We found that, in our trust, scene times in central stabbings were about 29 minutes with no specialist involvement, and dropped to 19 minutes with a specialist on scene — a reduction of 38%.
Moreover, the triage to a major trauma centre improved from 37% to 81%.
Now, the study isn’t perfect and we should be cautious in transferring the findings to other trusts with different staffing and trauma models, but it certainly gives food for thought.
Why did our data show such a strong tendency for non-specialists to remain longer on scene?
Figure 2: Median total scene time in stab trauma (from Cowley et al., 2019)
In central penetrating trauma, where the patient is not in cardiac arrest, there is little that can be done in the pre-hospital environment, other than expose the patient, cover wounds (either ‘bleeding’ or ‘sucking’) and get moving.
We must resist the temptation to take lots of observations, to do a 12 lead ECG or ensure all AMPLE information is noted.
It is impossible to gauge the depth and severity of any wound from its external appearance and, given the general demographic of patient and their ability to compensate, they really need to be with a surgeon at a major trauma centre, rather than on the street or the back of our ambulance.
So why aren’t we doing it and what can be done to improve outcomes and reduce deaths from knife crime?
We propose that approach should be three-fold, and none are easy. Firstly, we need to continue to educate ourselves.
Applying pressure to a penetrating wound
At the moment it seems clear that the presence of a specialist improves the situation, so tasking models should ensure they continue to be dispatched wherever possible.
In addition, we need to continue to spread the message of minimal interventions and reduced scene times — empowering our staff to do what the patient needs, and take them where they need to go, rather than the ‘complete obs and paperwork’ approach that is used on most incidents.
We must continue to train harder or, perhaps, just more efficiently.
As technology improves it may become easier and easier to fully immerse our staff in training incidents — certainly the improved accessibility and sophistication of Virtual Reality systems may mean that the non- technical aspects of these incidents, which are normally so hard to recreate, become that bit more reproducible.
However, this can only be one part of it — there is simply not the exposure or training capacity for non-specialists in these highly dynamic situations to expect perfect performance every time. That is not fair.
So, perhaps a more ‘out of the box’ approach is needed?
Some interesting evidence emerged last year showing that victims of penetrating trauma that presented at hospital by alternative means (e.g. private vehicle, taxi, police car) had a significantly lower likelihood of death than those brought in by ambulance (Wandling et al., 2018).
Admittedly, it’s not directly transferrable due to the setting of the study, but there are not infrequent reports of patients deteriorating in taxis and police cars whilst waiting for an ambulance, when a hospital is close by.
It would need a step change in attitudes surrounding the 999 culture, but police medics are an increasing part of their service and so it is not beyond the realms of possibility to develop a system where they are the conveying resource when an ambulance is not on scene.
Simulated SCAS trauma scene
Finally, the most obvious one is to stop people stabbing each other in the first place.
The Serious Violence Strategy was announced almost two years ago by the Home Secretary and, whilst it will take time to assess its impact, the pessimists amongst us will feel it is unlikely to solve the problem.
The vast majority of knife injuries are due to crime, drugs, mental health or, most likely, a combination of all three.
To suggest these are easily addressed would be optimistic to the point of naive, but people are trying and perhaps one of the most interesting, and promising interventions right now is the work of organisations like Redthread (many others are available) who, amongst other work, target the victims of knife crime when at their most ‘vulnerable’, often when lying in the resuscitation room with an unclear prognosis.
Their current reach is across hospitals in three of our major cities but it would be good to think that, in time, this reach will grow and perhaps they could move their focus from the resus room to the ambulance?
In summary, penetrating trauma kills quickly and subtly and, like so much serious crime, affects many more people than just the ‘patient’. It will occur more and more in the foreseeable future.
If you haven’t encountered it yet, you will. If you do encounter it, you will see it more often.
We need to be ready; we need to empower ourselves to do the bare minimum and quickly move to an appropriate hospital.
Perhaps, most of all, we need to continue to develop the wider system to minimise the impact and, eventually, put the numbers back on a downward trend.
References
1) Allen G., Audickas, L., Loft, P., Bellis, A. (2019) Knife crime in England and Wales. House of Commons Library (SN4304). 2) Cowley, A., Durham, M., Aldred, D., Crabb, R., Crouch, P., Heywood, A., McBride, A., Williams, J., Lyon, R. (2019) Presence of a pre-hospital enhanced care team reduces on scene time and improves triage compliance for stab trauma, Scan J Trauma Res Emerg Med 27:86. 3) Henderson,T.,Endacott,R.,Marsden,J.,Black, S. (2019) Examing the type and frequency of incidents attended by UK paramedics, J Para Prac 11:9. 4) Wandling, M.W., Nathens, A.B., Shapiro, M.B., Haut, E.R. (2018) Association of Prehospital Mode of Transport With Mortality in Penetrating Trauma: A Trauma System-Level Assessment of Private Vehicle Transportation vs. Ground Emergency Medical Services, JAMA Sug, 153:2.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-06 10:54:252020-03-06 13:19:34The Cutting Edge of Knife Crime: Time to Sharpen Up
By Anna Joval, Advisor, Humanitarian Values and International Law Unit, Norwegian Red Cross Published in Ambulance Today, Spring 2020, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
Imagine an ordinary day at work. The coffee is fresh, and you wait for your next assignment. Then it happens.
The disaster alarm goes off and it is yours and your teams’ responsibility to respond. It could be a natural disaster or a terrorist attack.
Hundreds, maybe thousands of people, are affected. Hundreds may need health care; many may already have lost their lives. Civilians are already at the scene facing the calamity.
In these circumstances, one can easily be overwhelmed by the magnitude of the situation, but at the same time the EMS personnel are trained to respond to emergencies, no matter how small or big they are.
It is in our backbone to always provide medical care and offer help.
The above imaginary scenario is no longer unthinkable, and the reality is that you, as a first responder, one day could be the one on duty when the alarm goes off on a massive disaster or a critical security incident.
This article will introduce you to the NO-FEAR project1 (Network Of practitioners For Emergency medicAl systems and cRitical care) and describes some of the challenges associated with bystanders and non-organized volunteers, whilst outlining how you can engage with the project activities.
The NO-FEAR Project
EMS plays a vital role in assisting wounded and sick people after security incidents.
However, there are several challenges that need to be addressed. As a response to these challenges, the pan-European NO-FEAR project was launched in 2018.
This coordination and support action project brings EMS, suppliers, academia, decision makers and policy makers together to collaborate and exchange knowledge, good practices and identify lessons learned.
Many of the NO-FEAR partners are practitioners who were directly involved in the terrorist incidents in Paris, Nice, Berlin, Madrid and Barcelona.
Based on their experiences, the consortium initiated the project to better prepare and respond to several challenges that EMS face, and to overcome difficulties, such as:
• A fragmented chain of actors responding to security related incidents.
• A need for actors to respond to new threats such as terrorism and armed convicts.
• A lack of
communication between the practitioners working in the eld and suppliers
providing goods and services.
• No common
methodologies and standardised actions.
The threat and risk situations today are quite different from just a few years ago, and security and preparedness plans are constantly being adapted to respond to new challenges.
Cross-border collaboration to develop a common understanding of the innovation potential gives this project a unique opportunity to improve the capabilities of EMS to respond to new threats, and assist casualties after security incidents.
This in turn will fill operational gaps and identify areas for future research, making EMS more resilient.
A higher frequency of natural disasters, critical security incidents and terrorist attacks are a growing trend in Europe and beyond.
The correlative rescue work is unpredictable, challenging and involves well known dilemmas and potentially dangerous situations.
When disaster strikes, we must be prepared, but what about the people already on site – the bystanders?
Civilians:
The First to Save Lives
Bystanders and non-organized volunteers usually initiate life-saving measures quickly. It is a misconception that people become helpless or panic during a crisis.
Although one may be affected by fear, the desire to help is stronger. The official report after the shootings at Utøya in Norway, 22nd of July 20112 points out what a valuable resource the ordinary man and woman are when disaster strikes.
Image courtesy of Martin Chico, Yemen
At Utøya, in addition to logistics on water, civilians also performed first aid, provided warm blankets and clothing, and showed tremendous care and compassion.
In the minutes following a critical incident, there will normally only be the wounded and bystanders on site before the police and EMS arrive.
These minutes can be critical for severely injured people and can mean the difference between life and death. Bystanders who understand the urgency of the situation may feel an immense responsibility.
Getting an overview of the situation and simultaneously trying to save lives with minimal resources contributes to additional stress3.
Reports tell the story of former bystanders who say that leaving someone behind is not an option, even with a “great personal risk and subsequent injury”4.
When the shootings at Utøya started, it did not take long before people at the landside understood that something was wrong. They heard gunshots and saw youths jump into the water, swimming for their lives.
We have also learned from the reports that young survivors from Utøya tried to help friends escape the gunshots.
Residents on the landside and camping guests collaborated to rescue the hypothermic and injured teenagers.
Whilst the youths immediately started to help each other, the residents and the camping guests got their boats on the water and went out to rescue the cold and injured teenagers. Some of the volunteers were shot at while saving lives2.
Image courtesy of ICRC Syria
Nevertheless, they kept transporting injured persons to the mainland. These volunteer efforts continued for some time after the police and EMS had arrived.
At some point, volunteers even provided water transportation for the police. Later they said: “the collaboration with the professionals was good, but it took them a long time to arrive”5.
The concern is not about people’s willingness to contribute when disaster strikes, but whether there should be limitations to what actions one can expect from bystanders.
Although it is sometimes necessary for first responders to make use of bystanders and non-organized volunteers to effectively meet the needs of the injured, the ethical reflections around whether professional responders put non-professionals in harm’s way, either physically or emotionally, must be taken into consideration and further discussed.
Given the unpredictable nature of any crisis, we understand that being near or on the site of the incident involves personal risks, but EMS has a duty to act, balanced by a duty to consider relative risk6.
At the end of the day, we are the ones who need to prepare for, and gain knowledge of, how to leverage bystanders and non-organized civilians as medical force multipliers during MCIs (mass casualty incidents)4.
The
Perception of the Bystanders’ Efforts?
Even those who work with adverse events may perceive a crisis as surprising and threatening. At the same time, they are expected to make decisions very quickly and with overwhelming pressure7.
Hence, it is not difficult to understand if and why professional first responders associate bystanders with increased chaos and stress, rather than as essential resources in the rescue work.
Mexico City: People helping after the earthquake. Shutterstock.
However, research8 has previously shown that the inherent altruism of the population is crucial to the efforts made to save lives under acute incidents.
This selfless concern for the wellbeing of others may explain why people help each other, carry out life-saving measures and stand together in times of crisis. Empirical evidence suggests that the civilian population can provide valuable resources which have not been fully utilized.
One reason may be the argument that when many want to “do well”, chaos and ambiguity can arise, which in turn can be problematic for the professionals8.
One cannot stop people from arriving to offer help, but too many people with the desire to contribute can also be a burden and an obstacle to the professionals doing their job.
This can lead to negative attitudes and wrong assumptions towards the bystanders. Nevertheless, we know that it takes time for professionals to respond to critical incidents and, in the immediate aftermath, the affected must rely on themselves.
Bystanders and non-organized volunteers can and should be considered a resource in crises, from which EMS can benefit.
By coordinating efforts and eventually taking over full responsibility, the information and work already carried out can be utilized for:
• A better
understanding of the situation.
• Efficient
and correct crisis management.
• A better
outcome for both lives saved and psychosocial aspects following the disaster.
This form of crisis management is based on collaboration to achieve control of the situation7. However, it is important to keep in mind that each crisis is unique.
The affected will have varying degrees of knowledge and needs, thus presenting different reactions to a situation.
Raising awareness of the inevitable interaction between the EMS and bystanders is crucial in achieving a better understanding of the value each group has when joining efforts to save lives.
National guidelines for establishing easily available first-aid courses to the public could be a way of strengthening the societal resilience.
But first and foremost, it is important that training in managing the bystanders and non-organized are embedded in a standardized education for EMS.
There will always be civilians who are first at the scene of injury and in many cases initiate life-saving measures, sometimes also further safeguarding the disaster area.
As a resource, bystanders are currently not fully exploited, meaning a considerable potential for strengthening society for emergency purposes remains to be utilised.
To contact Anna and find out more about the NO-FEAR project, you can email her at: [email protected]
References:
1http://no-fearproject.eu/ 2 Departementenes servicesenter Informasjonsforvaltning. (2012). Rapport fra 22. juli- kommisjonen (NOU 2012:14). Oslo: Departementenes servicesenter. 3 Kruke, B. I. (2012). Samfunnssikkerhet og krisehåndtering: Relevans for 22. juli 2011. Notat: 7/12. Risikostyring og samfunnssikkerhet, Krisehåndtering, 4 Universitetet i Stavanger. https://www.jems.com/2016/08/01/leveraging-bystanders-as-medical-force-multipliers-during-mcis/ 5 Haug, C.S. & Folvik, A. E. (2011, 24. juli). Han reddet 20-30 ungdommer fra terroristene på Utøya. Dagbladet. http://www.dagbladet.no/2011/07/24/nyheter/innenriks/terror/utoya/anders_behring_breivik/17436710/ 6 https://www.jems.com/2018/11/13/safety-is-third-not-first-and-we-all-know-it-should-be/ 7 Rosenthal, U., Boin, R. A. & Comfort, L. K. (2001) “The changing world of crisis and crisis management”. I: Rosenthal, U., Boin, R. A. & Comfort, L. K. (Eds.) Managing crises: threaths, dilemmas, opportunities. Spring eld III., Charles C. Thomas. 8 Helsloot, I. & Ruitenberg, A. (2004). Citizen Response to Disasters: a Survey of Literature and Some Practical Implications. Journal of contingencies and crisis management, 12 (3), s. 98-111. http://www.researchgate.net/publication/227847952_Citizen_Response_to_Disasters_a_Survey_of_Literature_and_Some_ Practical_Implications?enrichId=rgreq-8ae3e470-bb43-42ed-82ba-79145833939d&enrichSource=Y292ZXJQYWdlOzIyNzg0Nzk1MjtBUzoxMzE1MjIzOTY5NTQ2MjRAMTQwODM2ODc5MTI1NQ%3D%3D&el=1_x_2
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-06 04:15:272020-03-06 12:11:12NO-FEAR! First Responders at the Frontline: Collaborating with the Non-Professionals
An Interview with Tony Walker, CEO, Ambulance Victoria. Published in Ambulance Today, Spring 2020, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
As the world looked on in disbelief at the devastating Australian bush fires earlier this year, the Emergency Response teams were working day and night to reduce casualties amidst extremely challenging circumstances.
Tony Walker, CEO at Ambulance Victoria, gives us an insight into what effects the fires had on the Australian Ambulance Services and how the effects of climate change are shaping Ambulance Victoria’s response systems.
Harry
Squire (H.S): Tony, working within EMS can be challenging at the best of times.
How did the bush fires in Australia effect the ambulance service?
Tony Walker (T.W): The scale and intensity of the recent bush fires in Victoria was unprecedented, and their impact on our people and operations significant.
Ambulance Victoria’s Emergency Operations Centre coordinated a state-wide ambulance response.
The fires burned an area equivalent to two thirds of the UK. Entire towns were lost. Smoke turned day into night.
The remoteness of some impacted communities meant our teams were managing a challenging logistical and operational environment on a daily basis.
We had local
crews in the fire-effected areas and, as need increased, dispatched extra
paramedics to these areas where they worked along-side government-funded
medical officers and an Australian Defence Force medical team to ensure we had
adequate coverage on the ground.
We were
heavily involved in the relocation of vulnerable community members from local
hospitals and aged care facilities, and as people were being evacuated by the
Navy we provided the facilities of our Air Ambulance base back in Melbourne.
As smoke from the fires blanketed our larger cities and air quality plummeted to hazardous levels, we saw a 51% spike in calls for help for breathing problems in one night.
Many of those patients were taken to hospital, putting enormous strain on emergency departments.
Ensuring the safety of our staff was paramount. A number of ambulance crews were isolated in their communities, and there were other areas in which we couldn’t respond to emergency calls because fires made them inaccessible.
In the course of caring for their communities, some of our people lost their own families’ homes to the fires.
I’ve since spent time in some of the worst hit parts of Victoria, including the coastal town of Mallacoota where you saw in media reports the thousands of holiday makers evacuated to the beach.
I spoke to many of our people who have been at the heart of emergency and recovery efforts. Particularly for fire fighters, most of whom are volunteers, but also for my people, it’s been a long and difficult summer.
And I do feel a deep personal obligation to care for them. We created a special Bush re Support package to make available extra psychological support services and financial relief. Over 200 staff have utilised the scheme.
H.S: Bush fires
in Australia clearly aren’t anything new, and it does seem to me like the response
was well orchestrated and efficient, however, with extreme weather cases like
this seemingly becoming more frequent, are you worried for the future?
T.W: There’s no question
that climate change-induced extreme weather events are becoming more frequent
and more intense. The science has been forecasting this for three decades.
Personally, of course I am concerned for the world my generation is leaving to my children. My daughter Lucy is only four years old. I am grandfather to two-year-old Ella, and have another grandchild on the way.
Outside of the Mallacoota branch
I think this summer’s fires sheeted home to most Australians the impact of a warming world in a way that melting glaciers and stranded polar bears had not.
At Ambulance Victoria, our vision is to transition over the next five years to 100% renewable energy, reducing our emissions by 27%.
As you’d anticipate, carbon emissions from our fleet are a significant contributor to our carbon footprint, but we are not shying away from that challenge.
H.S: It’s a good point, I think we are all guilty at some level of feeling far-removed from the impacts of climate change, but when it hits on a personal level — it hits hard.
Are the Australian ambulance services prepared for another event like this? And do you think any lessons have been learned from this year?
Paramedics at Mallacoota
T.W: Extreme heat,
thunderstorm asthma, prolonged drought, fires, floods — extreme weather events
are coming down the road to challenge and change us at Ambulance Victoria.
Emergency services here learned a lot from the Black Saturday fires in 2009 when 173 people perished. As a consequence, this summer many lives were saved thanks to the public’s and emergency services’ greater understanding of the threat level and how to respond.
We learned a lot in 2016 when we experienced the world’s largest and most catastrophic epidemic of thunderstorm asthma.
Over a period of 30 hours, there was a 67.2% increase in respiratory-related emergencies. People died, ten people. It’s inevitable that we’ll be challenged again.
We need to be ahead. To future-proof our service, we need to think smarter, not bigger. We need to do things in more efficient and innovative ways.
Technology is enabling us to re-imagine and transform our service. We’re working proactively and in partnership with communities to build their capacity to respond to health emergencies.
Being ahead
means that we will be in a position to manage extreme weather events on top of
the significant demand drivers like mental health and an aging population that
are the daily reality in a modern ambulance service.
H.S: It is certainly a challenging time for EMS, especially in Australia, but it does seem Ambulance Victoria are managing these challenges well and planning for an inevitably more challenging future.
Is there a message you would like to give in general to the people in Australia involved in the emergency services?
T.W: There has never been a more challenging and rewarding time to be an emergency services professional.
H.S: Thank you for your time and insights, Tony. I think I speak for most people when I say the response to the bush fires by the Emergency Services in Australia has been incredible, and it certainly sounds like you’re geared up for climate-related response.
Personally, with this becoming a global issue, I think that there is a lot to learn from the work that Ambulance Victoria has been doing and is planning to do in the future and it will be interesting to see how things develop in the coming years.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-06 02:30:272020-03-06 13:16:39Global Warning for EMS
This article
has been reproduced with permission for Ambulance Today by NAEMT and is
also featured in NAEMT’s own publication, NAEMT Pulse Spring 2020 .
Published in Ambulance Today, Spring 2020, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
The 3rd edition Advanced Medical Life Support (AMLS) textbook was recently published, featuring new chapters covering critical illnesses which EMS practitioners often encounter in the field.
In this edition of Ambulance Today, Dr. Stein Bronsky, emergency physician and medical director for the Colorado Springs Fire Department and American Medical Response (AMR) in El Paso County, Colorado, discusses pharmacology in the field of EMS.
Bronsky is a contributing author of the new AMLS chapter on pharmacology.
Q. Before
we talk about pharmacology, can you tell us what got you interested in EMS?
When I was 17 years old, I got in a car accident – a bad car accident. I was driving and I fell asleep on a really narrow canyon road, the kind where if you swerve you may go off the edge of the cliff.
A bus driver saw us swerve. He sped up, swung wide and hit us to plow us up against the canyon wall and keep us from falling off the edge. I don’t remember a lot, but I remember having to be extricated.
I had a lot of broken bones. I almost lost my lower leg, and I had a head injury. I didn’t have any internal organ damage, but my passenger did.
The emergency crews knew how to handle the situation, and it was really impressive. I became an EMT shortly after that, and worked as a ski patroller in Utah while I was in college.
Q. Did you
always plan on eventually becoming a doctor?
No. My dad is
a pediatric immunologist and I wanted to do something different, so I went to
Israel to study Middle Eastern studies.
But while I was there, I became a paramedic. During the late 80s and early 90s, there was a lot of trauma there. There were an unbelievable number of car accidents.
They didn’t have traffic police, so there was nobody stopping anyone for speeding or driving poorly.
There were also terrorist attacks – mostly suicide bombers and backpacks left in crowded tourist areas, loaded with explosives.
They would just wait for somebody to pick up the backpack, and boom.
Israel got very, very good at MCI triage and treatment.
One thing they learned is that people will not stick around and wait to be triaged or wait for an ambulance.
If they can get up and physically move away from a scene, they will get as far away as possible. It’s human nature. If they are too injured, the people around them will pick them up and extricate them out of that circumstance.
Israel learned emergency crews will not get there in time to treat the majority of patients. There may be somebody who freezes up and doesn’t move, or who looks dead but is not quite dead and so people left them.
But it is single digit percentages of people who are still at the scene when EMS arrives, and who are still alive so you can do anything to try to save them.
Nearly all of the action is at the nearest hospital. Not a trauma center, and not the place best equipped to help them, but whichever hospital happens to be the closest. After my time in Israel, I knew I wanted to go to medical school and become an ER doctor.
Q. What do
EMS practitioners need to learn about pharmacology?
Pharmacology is the study of interactions between a medication and the human body. As an EMT or first responder, you learn practically nothing about pharmacology. When we get to paramedic school, we learn more.
But what we don’t really learn is the 10,000-foot view: what are the different classes of medications, why do we use them, what are our expectations when using one, and what are the effects, wanted and unwanted?
Opioids are a
perfect example. We want to alleviate the person’s pain but there are other
effects, including depressing respiration and lowering blood pressure. Those
are consequences we have to know about.
Typically, as eld providers, we receive a cache of drugs. You are taught about those specific drugs and when to give them.
But what happens if you don’t have one of those drugs because there is a shortage? How can providers make decisions about what to give when the situation requires critical thinking?
For example, let’s say you have a patient who has broken their leg versus one who has a huge, penetrating exsanguinating injury and their blood pressure is low.
You have to be able to use critical thinking – what is unique about this patient’s physiology and pathology? The drug I’m about to give for pain has some good effects and some bad. Is one of those bad effects something I need to worry about?
Let’s say you
have morphine, fentanyl and ketamine. Which one would you give to a patient who
is elderly, hypotensive, has an unstable pelvis after a fall and is in a lot of
pain, vs. somebody who is young and healthy with a pinned limb who needs to be
extricated?
I may give ketamine to somebody who is young, healthy and needs pain management during a prolonged extraction. You may have difficulty getting to them.
Fentanyl is short-acting and you may need to multi-dose the patient and monitor their respiratory drive or give supplemental oxygen, which may not be possible.
Ketamine would manage their pain and be a hemodynamically stable drug that does not affect the respiratory drive. Ketamine lasts longer and the dissociative effects of ketamine may be a good thing if you have to do an amputation.
But for an elderly patient with a broken pelvis, we want to use a pain medicine that will not lower blood pressure. Morphine and hydromorphone (Dilaudid) are out.
Could I use ketamine? I could, but ketamine has unpredictable side effects in elderly patients. Sometimes it works fabulously, but occasionally patients become unresponsive even with a small dose.
So we need to be very, very cautious and use critical thinking to assess which drugs are best in a given situation.
Q. What
steps can EMS practitioners take to avoid medication errors?
Dosing errors are the most common errors made on patients outside and inside the hospital. To reduce these errors, we need good, systematic communication, and methods of organizing our system.
Hospitals have set up extremely elaborate programs to make sure you are giving the right dose, and the right medication, to the right person. In the field, we don’t necessarily have those systems in place yet.
In Colorado Springs, we’ve taken some steps to mitigate that, such as standardized doses.
We have also gone to volume-based dosing for pediatrics, so you don’t have to do the math. Math is not most people’s strong point, especially not at 3 a.m. when you’re exhausted.
We also ask everybody at our agency to tell us when there is a medication error. This is a non-punitive process. We want to understand how we set you up for that failure and change our system so it doesn’t happen again.
Q. There’s a lot of concern about opioid addiction and the overuse of opioids.
In the EMS setting, is there a greater risk of EMS overtreating pain or undertreating pain?
We have gone from potentially over-treating pain, to now potentially undertreating pain because of concerns about opioids. Today we have a greater recognition of the potentially harmful side effects of the acute use of opioids, as well as the addictive properties.
One positive change coming out of this is that we have started to think about other possibilities for pain management, such as acetaminophen (oral and intravenous), NSAIDs (nonsteroidal anti-inflammatory drug) and ketamine.
We also need to consider the hazards of opioid medication diversion. Traditionally there isn’t a great chain of custody for controlled substances in the EMS system.
It behooves everybody to ensure they have systems to track these medications so we can reduce diversion and, if diverted, have a better chance of figuring out how it was diverted. Access to controlled substances is a risk factor for addiction.
Q. How can
bias impact pain management decisions?
Bias can be on opposite ends of a spectrum. Some providers may say, ‘I believe it’s our priority to make sure that every person who is experiencing pain is completely out of pain.’
Or you can have the opposite bias where you’d say, ‘I understand this person is in a lot of pain, but pain isn’t going to kill you. No way am I going to give an opiate medication. They can get opioids at the hospital.’
Cultural biases based on gender, socioeconomics, and race are also well-documented in the prehospital administration of pain medication.
Medics may be less likely to offer pain relief to a homeless person, or somebody they believe meets the picture of a drug-seeking person.
I don’t claim to have all the answers. But overcoming bias requires taking a really hard look at your personal beliefs and recognizing bias.
Although most people don’t self-reflect on this topic — they see their beliefs as facts and they don’t see another way of looking at it.
Q. Are
there pain management medications that you think are underused in the
prehospital setting?
I think there are several medications that are underused. As a culture in medicine, we think of opiates as the answer to pain management in emergency situations.
Almost all other medications and all other classes of medications are systematically and historically ignored as a possibility for treatment.
We need to do everything we can to broaden that view and determine when it is appropriate to use opiates and when it’s appropriate to use other types of medications.
Often in the prehospital environment, if a patient is deemed to be in tremendous pain they get an opiate, and if they’re not in that much pain they don’t get anything. But we can do better.
Say somebody has severe strep laryngitis (strep throat). We don’t think of that as a life-threatening emergency, but it can cause a lot of pain.
It’s hard to swallow, so they don’t want to put anything in their mouth and they can become dehydrated. Does this kid or adult deserve pain management in the prehospital environment?
Yes, they do. We could use topical medications, such as topical or nebulized lidocaine, which would provide tremendous relief. Tylenol or an NSAID would also help.
Even for bone fractures, not everybody needs an opiate — especially kids who respond very, very well to acetaminophen and NSAIDS.
Adults do too, although they are more mentally inclined to think over-the-counter medication isn’t going to help, whereas kids haven’t formed those beliefs yet.
Q. Studies show that anaphylaxis is under-recognized and potentially undertreated in the prehospital setting.
What does EMS need to recognize about anaphylaxis and the use of epinephrine to treat it?
The emphasis
on recognizing anaphylaxis has traditionally centered around airway issues. If
your throat is closing up, you can’t swallow and you’re having a hard time
breathing — you’re having a bad allergic reaction and we want the provider to
use epinephrine.
Anaphylaxis is a systemic process that can manifest in different ways – and not always with throat swelling. If you’re thinking only about the respiratory system, you may be missing other systemic effects, such as a full body rash or hives.
GI issues are common; people who ingest an allergen may have nausea, vomiting or abdominal cramping. Wheezing may make EMS practitioners think more about albuterol than epinephrine, but wheezing may also be part of an anaphylactic reaction.
Hives, GI
issues, wheezing, hypotension – these kinds of symptoms should trigger using
more aggressive treatments, including epinephrine, as well as
histamine-blockers such as diphenhydramine (Benadryl) and famotidine (Pepcid).
From an
educational standpoint, we need to do a better job explaining what is happening
in the body during anaphylaxis, so EMS practitioners are not just focused on
the airway.
Some of this also involves changing the culture at EMS agencies. EMS practitioners are often taught to only give epinephrine when you are sure somebody is in anaphylaxis.
If the symptoms aren’t exactly what they were taught, they are afraid that if they give epinephrine they will get into trouble. That environment impedes people from using their brains to work through a situation.
In our system in Colorado, we promote the idea that if you think it’s the right thing to do, even though it doesn’t check all the little boxes, you write down your reasoning and the thought process you went through.
Even if you’re wrong, you’re not in trouble. Guess what? Doctors get it wrong at times too. We want you to think critically. Sometimes you will be wrong, but a lot of times you will be right.
By Joseph Heneghan, Editor Published in Ambulance Today, Autumn 2019, Issue 1, Volume 17, Global Warning and the Burning Issues at the Core of Prehospital Trauma Care
It is with much excitement that I welcome you all to this first edition of the year for Ambulance Today. I’m happy to say that this year has gotten off to a flying start with more genuinely fascinating content in the pipeline than we can probably t into each edition.
This first edition
of the year is largely dedicated to trauma care — as we always like to kick the
year off with an edition that our readers can get lost in — but, as ever, it
has also evolved into so much more.
Whilst we have
some highly intriguing articles on prehospital trauma care which make for
riveting reading and which will inevitably excite most into delving much
further into the topics they expound upon, I’m thrilled to say that we have a
wealth of articles delivering some highly fascinating developments in EMS from
around the world in areas outside of trauma care too.
To alight on these first and foremost, I’d like to draw your attention to Grant de Jongh’s article on the recent move by the National Police Chiefs Council to use the Health Practice Associates Council (HPA) register as a referral pathway for cases involving non-Paramedic ambulance staff.
To understand why this is such an important development and to appreciate what a positive leap forward this is for safeguarding patients, as well as the reputation of the various roles and professions within EMS, I can only implore you to read further but, suffice to say, the mission being undertaken by the HPA should be supported by all those who hold EMS and the Hippocratic ethos it is built upon dear to their hearts.
MSc Paramedic Science Course Leader, Phil Ashwell, from the University of West London details their new Pre- Reg course which was introduced last November.
The course has been thoughtfully tailored with every foundation of its creation carefully considering the many subtle factors which can affect students’ learning experiences and should offer some interesting approaches for anyone interested in education and development within EMS.
The Palestine Red Crescent Society has offered a second, deeply motivating interview which, when read in comparison to the first which was published within our previous edition of Ambulance Today, offers a deep understanding of the mechanisms of EMS delivery within Palestine and is sure to leave any EMS devotee feeling proud of their chosen vocation.
A world away for many of you, this piece still manages to hold a mirror up to you all, shining light on the quietly humble humanitarian paths you have chosen.
And, last but certainly by no means least, I am incredibly proud to present our Deputy Editor’s debut article with Ambulance Today.
Harry Squire has been with us for just over a year now and, for any of you who know our publication well… well, what a year it has been.
I can safely say that, without his keen intellect, his rapidly developed understanding of EMS and the psyche that forms it, and his burning passion for honest reporting based upon a proud and ethical respect for media and the service any publication must offer its readership, we would not have been able to pursue half of the illuminating and progressive content which we were able to provide you all with last year.
True to form, he has offered an eye-opening interview with Ambulance Victoria’s Chief Executive, Tony Walker, on the difficulties that the recent Australian bush fires have posed to their delivery of EMS and how those difficulties have been met.
Using this as an example, he poses a question which all EMS leaders across the Globe, without exception, must ask if services are to prepare themselves with foresight for the changes in our environment that lie ahead and which will inevitably affect how EMS is delivered for many parts of the world.
If we do not take stock of the different environments we are bound to and the warning signs they are currently offering, then I fear that the obstacles they will later present will come as a very sudden and unwelcome surprise. It is a discussion I hope to see much more of within the Global EMS community.
But, as much as I would love to take you on a tour of every article within this edition, there is simply too much content and yet not enough space for me to do so.
Articles such as Alan Cowley’s reflection on the growth of knife crime and penetrating trauma in the field and NAEMT’s interview with Dr Stein Bronsky on the vital importance of the Paramedic’s understanding of pharmacology will certainly leave you glued to the page.
I can safely say that I sat with great interest as I worked through these articles in the composition of this edition and enjoyed them immensely.
Not to mention Anna Joval’s piece from the Norwegian Red Cross on how bystanders can, and should, be utilised during MCI’s for a wealth of practical reasons — this one offers much food for thought and is of great use to anyone, from Operations Directors right down to those working regularly in the field on a daily basis. Its applications are many.
And still, we have so much more from our usual contributors; I really feel guilty that I cannot continue.
You’ll just have to see for yourselves, but I’m sure you’ll gain as much enjoyment in doing so as I did myself.
In the meantime, I wish you all a pleasant start to the Spring.
If I have noticed one thing so far this year in the compilation of this edition, it’s that there are a great number of highly fascinating and innovative discussions taking place around the world in EMS and their exploration seems to promise an interesting year ahead!
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2020-03-05 23:22:382020-03-05 23:34:00Well of Content, Spring of Knowledge
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, you cannot refuse them without impacting how our site functions. You can block or delete them by changing your browser settings and force blocking all cookies on this website.
Google Analytics Cookies
These cookies collect information that is used either in aggregate form to help us understand how our website is being used or how effective our marketing campaigns are, or to help us customize our website and application for you in order to enhance your experience.
If you do not want that we track your visist to our site you can disable tracking in your browser here:
Other external services
We also use different external services like Google Webfonts, Google Maps and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.