Construction work on the new state-of-the-art, £3.9million helipad at Manchester University NHS Foundation Trust (MFT) has begun and is set to benefit four major hospitals in Manchester city-centre.
The new helicopter landing site, being built on the roof of Grafton Street car park on Oxford Road will enable critically ill or injured babies, children and adults to be airlifted straight to four major MFT hospitals.
A high-level patient transfer corridor will connect the helipad landing site to Manchester Royal Infirmary (MRI), Royal Manchester Children’s Hospital (RMCH), Saint Mary’s Hospital (SMH) and Manchester Royal Eye Hospital (MREH).
Each of the hospitals on MFT’s Oxford Road Campus offer world-leading, specialist services which are not always available at other hospitals within the North West and in some cases, the rest of the UK. The construction of the helipad is expected to see an estimated 312 patients airlifted to the site each year.
Funding for the helipad was raised by MFT Charity’s Time Save Lives Appeal, which raised a phenomenal £3.9million in just 12 months, thanks to the dedication and generosity of its supporters.
The Appeal was the focus of the Charity’s fundraising, with individuals, businesses and community groups from across the North West all showing their support. This included a generous donation of £1.3million from the HELP Appeal and £1.1million from the government’s LIBOR fines funds in the Chancellor’s Budget.
Building work officially began earlier in June 2019 and the helipad is set to be fully operational by spring 2020.
Artist impression of the Helipad
Robert Bertram, Chief Executive of the HELP Appeal added:“This is one of the biggest donations that the HELP Appeal has given to any hospital. But, we didn’t hesitate in coming to their aid, because as the Major Trauma Centre for the northwest, a life-saving helipad is essential. We are delighted that its construction is now underway because it will save time and save lives.”
Manchester University NHS Foundation Trust Chairman, Kathy Cowell, said: “I am delighted that the construction work has begun and that we will be able to offer this service in spring 2020. It is a very exciting time for MFT and the helipad is an amazing project which will help to save so many lives in Greater Manchester, the North West and beyond.”
The first 60 minutes following a major trauma injury is known as the ‘Golden Hour’ and treatment within the first hour can mean the difference between life and death.
Dr Jon Simpson, Medical Director and Consultant Physician at Manchester Royal Infirmary, added: “The quality and speed of specialist medical care following a major trauma injury is vital to ensuring our patients have the best chance of a full recovery. In these situations, patients need to be transferred to a Major Trauma Centre or an Emergency Department, both of which we have on site at the MRI and RMCH.
“The construction of the helipad will be invaluable to us and our patients as in some situations; the quickest or most appropriate way to get a patient to these services is by helicopter. The ease of access to these specialist services once the helipad is fully operational will allow our hospitals to save many more lives and increase the chances of a full or improved level of recovery for our patients.”
The 130m-long bridge between Grafton Street car park and MFT hospitals will be suspended 19 metres above street-level with direct access to MFT hospital facilities such as 24 hour Emergency Departments, a Major Trauma Centre for children and a 24 hour a High Dependency Obstetrics Unit.
Construction of the helipad on the roof of the car park has been carefully planned to minimise disruption to MFT staff, patients, visitors and other site users.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-13 12:07:522019-08-13 12:07:55Construction work has begun on the first helipad of its kind in central Manchester
Families facing death and bereavement at St Mary’s Hospital now have access to specially trained volunteers from Mountbatten, who can offer dedicated time to support people during this challenging time.
The ‘end of life care companions’ have been carefully selected and given comprehensive training by experts in end of life care at Mountbatten, who are working with the Isle of Wight NHS Trust to improve support to people in hospital who are dying, as well as to their loved ones.
Liz Arnold, Director of Nursing at Mountbatten, said: “It is recognised that ensuring one-to-one, dedicated support for patients who die in hospital can be challenging in such a busy environment. By training our volunteers in areas including communication skills and bereavement support, we hope to be able to offer comfort, reassurance and a listening ear to both patients and their families. Through our volunteers, we are also able to explain more about our specialist bereavement service which is open to anyone, wherever a death may have occurred.”
Shane Moody, the trust’s Clinical Director for End of Life Care and Consultant Nurse for Critical Care and End of Life Care said “Thanks to working in partnership with Mountbatten, we are able to provide this new service within the acute hospital giving us another source of support for those at end of life and their families. If the scheme proves successful then we aim to recruit more End of Life Care Companions.”
Families or patients who feel they would like a companion to support them during their stay at St Mary’s Hospital should speak to a member of staff on the ward, who will then contact the Integrated Palliative and End of Life Care Team (available from 8am to 8pm, Monday to Friday).
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-13 11:54:102019-08-13 11:54:14Mountbatten trained volunteers to support patients dying in hospital
Ambulance staff from Bromsgrove Hub are joining forces with 999 colleagues later this month to help find a donor match for a little boy who urgently needs a transplant.
Bromsgrove-based Clinical Team Mentors Abi Coombs and Ruth Hodgson and Technician Caroline Hadley have been following the story of ‘Finn the Fabulous’; a seven-year-old boy called Finn Hill from Clent who has a rare and life-threatening condition where the immune system begins to damage a person’s own tissues and organs.
His only hope of a cure is a stem cell transplant from a perfectly matched donor which has led his family to work tirelessly to raise awareness about the condition as well as hold events to get people to register to be donors by doing a simple mouth swab.
Abi, Ruth and Caroline have now helped to organise a tri-service open day at Bromsgrove Fire and Police Station on Saturday 31stAugust, 12pm – 4pm, where people can come to sign up as a blood stem cell donor and have a swab taken in the hope of finding a perfect match for Finn.
Caroline said: “Finn’s story is one that has captured our attention and our hearts. Aged just seven, he’s been battling this condition for three years of his short life already. Organising ambulance representation at the tri-service open day is the least we could do to ensure Finn gets as much help as possible to find a stem cell match to save his life.”
If you aren’t already on the UK Stem Cell Register and are free on Saturday 31st August, please come along! Alternatively, you can visit the UK Stem Cell Register via dkms.org.uk or anthonynolan.org. To find out more about Finn the Fabulous, visit https://www.facebook.com/finnthefabulous/.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-13 11:35:542019-08-13 11:36:20TEAM 999 SET TO HELP FIND A DONOR MATCH FOR ‘FINN THE FABULOUS’
Published in: Autumn 2018 Edition of Ambulance Today Magazine
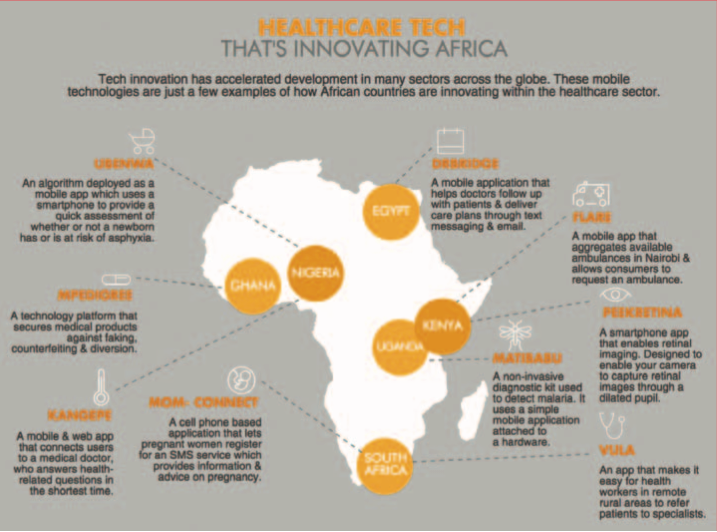
This Africa Quarterly editorial looks at the increasing demand for healthcare across the continent, and the pressures to reduce costs and show increases in value and patient care, including outcomes. Technology addresses key healthcare problems in developing economies and can also in turn add value. Small victories can lead to vast improvements.
Health systems are now rapidly developing and the Fourth Industrial Revolution in healthcare is upon us – wearable internet technology that will monitor our health in everyday life. Practitioners and patients can take full advantage of new and ubiquitous technologies. The smartphone in your pocket can open new avenues in healthcare.
Africa already uses technology to manage human resource constraints, such as text services that enable doctors to support Trained Birth Assistants at a distance. With rising economies and urbanization, noncommunicable diseases (NCDs) present new challenges to Africa’s emerging health systems. We believe that addressing Africa’s “dual-disease burden” of both NCDs and infectious diseases will require developing and adopting low-cost and high-quality medical systems that encourage people to manage their own health. Mobile technologies and new breakthroughs in customized care will help us succeed.
Patrice Matchaba, Head of Global Health and Corporate Responsibility, Novartis – WEF AGM 2018
Those of us with many years’
experience in EMS have then been privileged (or cursed) to see significant
changes across the board regarding equipment, patient care, protocols and drug
therapies. Many of us have actively pushed for change and new equipment; be it
about fluid therapy, bleeding control, pain management and airway management.
At times we miss the most crucial approach to patient care neatly summed up by
Hippocrates (400 BC approx.): Cure Sometimes. Treat Often. Comfort
Always.
The classic approach to patient care
has always been underpinned by the following:
• Arrive at a diagnosis by patient
consultation and physical hands-on examination
• Confirm one’s diagnosis via various
diagnostic devices
• Reaffirm one’s diagnosis by means of special investigations
Will technology change this approach, for better or for worse? Looking back at history, we see that not all new technologies have been readily accepted by the medical community. Many were viewed (/are viewed) with suspicion. In the 1930s some doctors doubted an X-ray image of the chest was as reliable as a physical examination. Devices threatened to replace the diagnostic expertise of the traditional doctor. Many doctors have valued their clinical experience over machine-produced information. Other technologies initially failed because doctors or patients found them impractical. The ECG was only useful when it became portable and reliable enough to be used at the patient’s bedside.
Drone carrying blood in Kigali
The entire patient/medical practitioner relationship is changing, as the patient has access to a wider range of medical information. Our patients are possibly smarter (maybe). Patients have access to more medical information with the result that, at times, they might be less trusting and prone to ask more questions of their medical practitioner. As practitioners we must be open to this new questioning patient and be willing to answer more questions than we did in the past.
Taking cognisance of all of the above: what is the healthcare practitioner to do?
There is an acknowledged gap in the “bench to bedside” cycle of medical discovery and its implementation in clinical practice, which can mean a gap of years changing “what we know” to “what we practice”. Hence the treatment of patients in an emergency setting should not only be concentrated on developing new technologies but must also involve proper training and skills development; medical talents needs to be honed. New technologies must always mandate new skill sets, protocols and procedures.
An area of import in medical development is patient information. The more patient information we have at hand, the more appropriate patient care can be rendered. Information and knowledge management is critical in helping with the decision-making process and thereby improving patient care.
Many medical practitioners believe that patients should take an active role in managing their own health information because it fosters personal responsibility and ownership, enabling both the patient and practitioner to track progress outside scheduled appointments and at times of a medical emergency.
Patient smart cards are a way to grapple with this issue of information. They will allow patients to upload their health records via a ash drive and carry their information with them in their wallet.
Information may be accessed through cloud-based storage and encrypted systems anywhere in the world or plugged into medical smart readers. Medical practitioners can update to cloud technology in real time and the patient’s own medical doctor can be alerted to changes in the cloud files. Ultimately, devices with communication and motion/health monitoring functions are expected to be implanted in the body. These changes are expected to help people manage their health more closely, and possibly allow medical practitioners to use this valuable data in emergencies.
Another key area where technology can aid is in having more information at our fingertips via a “differential” diagnosis or problem list, accessed via the cloud and linking to our patient and the further information we input. After reviewing the patient history and examination, the practitioner must then trawl his memory banks and innate knowledge base, or one may need to consult texts/online sources to check-up/confirm their thinking.
Cloud-based technology could aid us and speed up the confirmatory differential diagnosis. There is no doubt room for improvement in the current approach, with many practitioners currently relying on their tacit knowledge base at the frontline which, while mostly effective, is subject to human error. Once the differential diagnosis or problem list is drawn up, then a related treatment plan can be formulated, and treatment in the form of procedures and/or prescriptions for medications may be suggested by our cloud database.
We need to focus on leveraging the information we have and if we do not pay enough attention to building a basic infrastructure, we will be unable to make the Fourth Industrial Revolution a reality.
Emergency Medicine must continue its current academic trajectory, to keep pace with the challenges that technology brings to our patient care. If academic training lags behind the technology curve, our practitioners and therefore our patients will be the poorer. We must ensure that there is no technology/practitioner gap, as we continue to push the boundaries in improving our patient care.
The danger of technology is that it can make us lazy and reliant. It has become noticeable in certain areas of emergency medicine how our reliance on technology has allowed us to forget the three cornerstones of good medicine; diagnosis, confirmation and reaffirmation, of which the diagnosis and confirmation are reliant on us having a hands-on approach to our patients (which is becoming a dying art). Good solid diagnostic skills will always be an essential tool of medicine, especially emergency medicine – we forget this at our and our patients’ peril.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-12 13:17:492019-08-13 11:12:25Clinical innovation and technology in medicine and its challenges
Published in: Autumn 2018 Edition of Ambulance Today Magazine
Mechanical cardio pulmonary resuscitation (CPR) has promised to improve outcomes for patients in both hospital and out of hospital setting by improving the quality and consistency of CPR, essential in improving survival rates from cardiac arrest. The efficacy of mechanical CPR has been evidenced in laboratory conditions and staged testing. Results showed more consistent refractory periods, more consistent depth and rate, and when used in a moving vehicle potentially remove the need for paramedics to ride unrestrained. While it is likely that mechanical CPR devices have a role to play in pre-hospital medicine where manual CPR is not possible, difficult or as a bridge to advanced therapies, there are still questions on their role other than in very specific situations and in relation to patient outcomes.
However, despite questions about the clinical effectiveness of mechanical CPR devices many EMS systems and First Responder organizations are deploying these expensive items to an increasing number of ambulances and responder units for general use. In some cases, more effective and evidenced-informed interventions1 may have not been implemented e.g. Telephone CPR, Public Accessible Defibrillator databases, crowd sourced bystander CPR applications and public CPR learning events.
This article looks at the evidence for implementation of a mechanical chest compression device in an EMS System, reviewing literature for both the PhysioControl LUCAS Chest Compression System2 and the ZOLL AutoPulse Resuscitation System3 mechanical CPR devices and is intended to start a conversation. However, an underlying question is that as EMS, either health-based or public safety-based, continues to grow and as we adopt new technologies, do we need to be more rigorous in assessing the clinical effectiveness of the devices we deploy?
To investigate the use of mechanical CPR here in the Canadian province of British Columbia we wanted to understand in more detail the evidence supporting mechanical CPR devices and in particular the LUCAS and AutoPulse devices. We wanted to develop internal BCEHS4 recommendations on the use of mechanical CPR devices as well as outlining areas where we felt more research is needed to support their wider use in pre-hospital medicine.
MARKETING OF MEDICAL DEVICES
Firstly, let’s discuss the marketing associated with medical devices. Manufacturers of medical devices and pharmaceuticals have spent many years honing their skills in selling products to medical professionals and not always to the patient’s good, as we have seen in the current opioid crisis. There is no suggestion of harm being caused on the scale of the current opioid crisis by the use of mechanical CPR devices, but a question: Are we as experienced in dealing with manufacturers as we think we are?
Both PhysioControl (LUCAS) and ZOLL (AutoPulse) as manufacturers have made easily-accessible materials available describing their products and how they can impact outcomes. Obviously, I must state openly for balance that my limited summary below of this information is biased as I have focused on contradictions in these materials. Some of the research quoted does offer support for the use of both LUCAS and AutoPulse in the management of out-of-hospital cardiac arrest. There is also no suggestion that any researchers involved in these trials were not transparent about their industry funding, contracts or positions within the manufacturer’s organizations. However, in my view there is currently no clear high-quality definitive evidence to suggest that mechanical CPR is superior to, or more effective than, manual CPR in a pre-hospital setting in these papers.
The LUCAS Bibliography5 summarises the PARAMEDIC6 trial telling us ‘…there was no evidence of improvement in 30-day survival with LUCAS 2 device compared with manual compressions, but it was noted that actual use of the LUCAS device in the LUCAS group was low’. However, it misses the finding: ‘The trial was unable to show any superiority of mechanical CPR and highlights the difficulties in training and implementation in a real-world EMS setting’.
The ZOLL website7 for AutoPulse makes a number of statements around efficacy of iA-CPR. The website includes the following statement: ‘Multiple trials confirm the AutoPulse is superior to manual CPR when it comes to increasing a patient’s odds of achieving return of spontaneous circulation (ROSC)’.
Of the papers referenced that support this, Steinmetz et al8 investigated the implementation of the 2005 European Resuscitation Council guidelines9. In this investigation data including AutoPulse use was only found in the second arm of the trial after the implementation of the new guidelines were made. In discussion investigators say: ‘We do not know what role the chest compression device played in relation to overall improvement in survival as the apparatus was only associated with improved ROSC at admission but a significantly worse 30 day survival rate. The chest compression device was only used in 77/419 of the cardiac arrests resuscitated. From this we can hardly claim that the AutoPulse was fully implemented in our unit’. Of those studies that did demonstrate improved outcomes for mechanical CPR included in this section of the Zoll website caveats included – ‘not statistically significant’10, ‘…research is needed to further define the value of LDB in resuscitation’11 or ‘…may improve the overall likelihood of sustained ROSC…’12.
The reason I highlight these cases, from both LUCAS and AutoPulse literature, is to highlight the need to evaluate the Class of Recommendations (i.e. strength) and the Level of Evidence (i.e. quality) of evidence we are given on interventions.
Evaluating clinical research using, for example, the AHA framework13 allows consideration of the Class of Recommendations. Language may include words such as ‘indicated/useful/effective/beneficial’ which are strong recommendations or ‘may/might be considered’ which are classed as weak recommendations. For Level of Evidence; Level A is high quality evidence from more than one RCT, while Level C-LD includes randomized or non-randomized observational or registry studies with limitations of design or execution and a lower level of evidence.
Our challenge is to evaluate all available evidence, in a framework that allows us to synthesis findings into a risk-based, decision-making process around the introduction of new technologies, procedures or medications. The point I want to make is this: Are we fully investigating the effectiveness of equipment being deployed or are we willing victims of marketing collateral?
LITERATURE REVIEW
Early Trials: Earlier porcine trials of the mechanical CPR devices14,15, conclude that they contributed to better circulation in resuscitation from Ventricular Fibrillation than manual CPR. A more recent study reported in the Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine16 also supported this finding using a load-distributing band that improved ventilation and hemodynamics in a porcine model of prolonged arrest. This study found that the use of LDB ‘…significantly improve the hemodynamics and respiratory parameters during resuscitation, dramatically producing greater passive ventilation, which can improve gas exchange during CPR…’
CPR quality during ambulance transport: A series case study17 on the quality of CPR in Europe (n176) found that chest compressions in out-of-hospital cardiac arrest (OHCA) were not delivered consistently and most were too shallow. ECG analysis and defibrillation accounted for only small parts of these gaps. A similar study comparing the LUCAS device and manual CPR using manikins undertook 16 simulated eight-minute ambulance transports18. In the transports using manual CPR there were variations in quality not seen in those involving the LUCAS device. The trial noted limitations but hypothesised that the LUCAS device was a reliable alternative to manual CPR in transport situations, stating that further clinical studies were required to inform this hypothesis.
Paramedic Safety: Provision of manual CPR in a moving vehicle is difficult and increases the risk of paramedic injury; however, there was limited research found in this area. In Hong Kong a study19 found that 60% of responding paramedics (n318) complained of discomfort when delivering CPR (in any setting), with a sub-cohort associating CPR to back injuries. The use of mechanical CPR devices for prolonged periods of CPR may reduce the risk of musculoskeletal injuries to paramedics and other emergency responders.
Patient Harm: Investigation into harm caused by L-CPR devices20 found that in patients with unsuccessful CPR following OHCA there was no difference in the incidence of sternal fractures compared to patients receiving manual CPR. While the study noted a higher rate of rib fracture, no injury sustained was found to be fatal. Paradis NA et al21. in an abstract for the California AutoPulse Quality Assurance Registry published in Circulation (2009) comments: ‘Adverse events are only rarely reported by EMS personnel and do appear more common in patients treated with the iA-CPR device’. Couper et al22. in their review of mechanical CPR suggest that there is no overall difference in injury rates caused by chest compressions in both the CIRC23 and LINC25 trials, but there are differences they say in the injury patterns. In all of these papers it is stressed that the instance of potential injury was low.
Patient Outcomes: Findings of a large US population-based study (n80861) into survival from OHCA was published in a CARES Research Letter24 (all types of mechanical CPR devices). It concluded that ‘mechanical CPR for routine cardiac arrest care was associated with worse outcomes’. Outcomes were based on survival rates (11.3% manual CPR, 7% mechanical CPR) and favourable neurological outcome survival (9.5% manual CPR, 5.6% mechanical CPR). It noted that data on the time of arrest, time of first CPR and timing of interventions were not reliably reported, including any delays in time to first de defibrillation. Importantly it also highlighted variations in the use of m-CPR across agencies. The median use was 43.9% (21.7% in >75% of responses and 37.7% in <25% of responses). Similar outcomes for both survival and neurological outcomes were evidenced where the use of mechanical CPR exceeded 50% of responses.
The LINC Randomized Trial25, funded by PhysioControl, was a multi-centre clinical trial (n2589) comparing manual CPR and LUCAS device with measures at 4hrs and secondary end points of survival at 6months and CPC score. During the trial changes were made to the resuscitation protocol for patients receiving mechanical CPR with an initial shock prior to analysis and 3min CPR cycles. A noticeable difference in study cohorts was the time to first defibrillation with the mechanical CPR cohort 90 seconds later than the manual CPR cohort. This trial concluded that mechanical CPR using the LUCAS device can be delivered without major complications with no difference in 4hr survival between groups. Researchers stated that mechanical CPR ‘…did not result in improved outcomes compared with manual chest compressions’ and that further investigation of the amended resuscitation protocol was needed.
The CIRC23 trial with centres in the US and Europe, compared manual CPR to mechanical CPR using AutoPulse. In the introduction the researchers acknowledged that mechanical CPR would never fully replace manual CPR however they state that ‘…there was a need for another randomized clinical trial comparing manual and integrated mechanical CPR, where a patient receives manual compressions while the mechanical device is deployed’. The trial enrolled n4753 patients with 49.6% (n2099) receiving CPR using AutoPulse and 50.4% (n2132) receiving manual CPR. The findings across all three measurements: sustained ROSC to ED (iA-CPR 28.6% vs manual CPR 32.3%); 24 hour survival (iA-CPR 21.8% vs manual CPR 25.0%) and to hospital discharge (iA-CPR 9.4% vs manual CPR 11%) met the criteria for equivalence (odds adjusted ration of 1.06).
The trial protocol, developed by ZOLL with the principal investigator, used a complicated double triangle statistical test design which in the author’s own words ‘…is unfamiliar to many in this field’. With this statistical model their conclusion that ‘…compared to high quality manual CPR, iA-CPR resulted in statistically equivalent survival to hospital discharge’ is supported in their findings.
The inclusion of the CIRC 23. trial in a subsequent meta-analysis, Gates et al26. has raised questions around the design, including missing neurological data at discharge and the exclusion of some data from one centre. The authors of this meta-analysis go as far as to suggest that ‘…the conclusion of “equivalence” in this situation is questionable’.
Wyer 27. in commentary of Bonnes et al 28. meta-analysis of randomized and observational studies reminds clinicians and researchers of well-established patterns of effect going on to say: ‘In OHCA, mechanical compression devices and other failed interventions…may restore cardiac function in the field and increase hospital admissions (and the cost of care) but are unlikely to improve patient survival to hospital discharge’. He suggests that: ‘Clinicians should look beyond new drugs and devices, focus on the basics of effective CPR, and await well-controlled clinical trials framed to test basic assumptions.
Neurological Outcomes: Most of the primary end points of trials for mechanical CPR have focused on ROSC. Arguments for this include variations in post-arrest treatments in hospital and post-resuscitative care. These trials have posited that this is the most appropriate measure of effectiveness for these devices, even when the period of ROSC is as low as one minute. Other trials have been poor at collecting neurological data with CIRC 23. missing 27% of data on this outcome at discharge in part due to the study design.
Newberry et al 30. explored this important measure and points to some interesting observations. Their retrospective observational study compared outcomes of n3,469 patients over a 36-month period. While their data showed mechanical CPR as being associated with poor neurological outcomes, once adjusted by logistical regression for confounding variables the outcomes were similar. They suggest that advanced airway management and medications may be the root cause of the poorer outcomes with higher rates of endotracheal intubation and epinephrine use with mechanical CPR devices. They suggest that current resuscitation protocols are developed around manual CPR and the greater efficiency of mechanical CPR may, for example, increase the toxicity of epinephrine. They suggest that due to these poor neurological outcomes: ‘The continued use of mechanical CPR devices should be limited until further investigation better defines the optimal medication dosages and airway management when mechanical CPR devices are utilized’.
DISCUSSION:
Early trials concluded improved consistency with the use of mechanical CPR and improved blood ow during CPR. These factors have not been disproved and subsequent trials have confirmed that these benefits are realistic. However, the advantages they should give during resuscitation have not been clearly evidenced in subsequent clinical trials and particularly in patient-oriented outcomes.
The risk of harm during transport for OHCA patients and paramedics alike has been mitigated significantly as protocols for discontinuation of resuscitation have been adopted. This has reduced the numbers of patients being transported to emergency departments with ongoing CPR in transit. However, for the small number of cardiac arrest patients with a treatable cause being transported this risk still exists. In addition, more at risk cardiac patients 31,32. are now being transported to specialized cardiac services by EMS based air critical care programs. With manual CPR being impossible in aircraft, cardiac arrest protocols for pre-flight application are now common.
While there is some evidence that mechanical CPR devices have caused injury to patients there does not appear to be a body of evidence to call on to support this as a significant factor in their use. In fact, in many cases manual CPR is given prior to the application of mechanical CPR and those injuries may have resulted from the manual CPR. Most of the research in this area, Couper 22. suggests, relies on autopsy and radiography which are not systematically collected or reported. The low level of evidence in this area coupled with the suggestion that there is a potential risk for some patients though cannot be ignored when considering wide spread deployment of these devices.
The CARES Research Letter 24. suggested potential adverse outcomes with low rates of mechanical CPR device application. However, survival and neurological outcomes for patients where the application of mechanical CPR devices was high was consistent with manual CPR, suggesting potential issues with training and confidence in their use. Many trials have raised the need for a comprehensive and ongoing training package to be linked to the use of mechanical CPR. CIRC 23. with its long lead in period and training program reported favourable outcomes. PARAMEDIC6 trial reported concerns around training and maintenance of competency in the use of mechanical CPR devices. During this trial (n4471) 40% of the mechanical CPR cohort did not receive mechanical CPR. Within this group 15% did not receive mechanical CPR ‘because of difficulties inherent with implementation of new equipment and the training and quality issues’, the conclusion recommended that ‘research should look to de ne the optimum method and frequency of such training’.
Targeted rather than general deployment could help with skills retention for practitioners, higher usage rates and allow for easy identification of any remedial training requirement.
The LINC Randomized Trial 25. demonstrated comparable outcomes but involved changes to resuscitation protocols for those receiving mechanical CPR with the authors suggesting further investigation into those changes. Newberry 30. also raises the question of the use of standard resuscitation protocols for mechanical CPR rather than amended protocols that may be better suited to their use. While this is supposition it may in some part explain why survival rates from mechanical CPR do not consistently match or better cases where manual CPR is provided.
RECOMMENDATIONS:
The review found no body of empirical evidence demonstrating improved survival rates associated with the use of mechanical CPR. However, there are occasions when manual CPR is ineffective and mechanical CPR has a place, including as a bridge to advanced therapies. Despite results not confirming the superiority of mechanical over manual CPR many researchers suggest exactly this conclusion while stressing the need for comprehensive training regimes. Taking these factors in to account we developed three internal BCEHS recommendations:
1. Mechanical CPR devices may be used in the following circumstances: transfers with medical/hospital teams; approved clinical trials; high angle patient rescue; confined space retrieval or transport e.g. airvac; hypothermic cardiac arrest retrieval and transport.
High quality manual CPR would be difficult in all these circumstances. The risk of re-arrest in some cases may be high and the pre-placement of a mechanical CPR device could be considered in confined spaces such as aircraft. Mechanical CPR devices may have been placed correctly by hospital teams prior to arrest or during advanced therapies e.g. ECPR and removing them would cause patient harm or the cessation of those therapies.
2. If already applied by an appropriately trained person and the number of responders does not allow for an appropriate rotation for HQ-CPR then the device can remain in situ until enough responders are available. In addition, if the patient is transported then it may be left in situ to reduce the risks associated with CPR in a moving vehicle.
One explanation for poorer survivability rates with mechanical CPR devices are delays in treatment while devices are applied. Removing them therefore may also cause further delays in treatment. Misplacement of devices or technical issues with them may raise the risk of injury to patients and delay other treatments, therefore requiring trained staff to travel with the patient. The numbers of patients being transported with CPR enroute is low and often this is with treatable causes e.g. post-trauma, immersion or hypothermic arrest. If CPR is indicated for treatment and a device has been applied unless high quality CPR is possible it should ideally not be removed.
3. The term ‘appropriately trained person’ includes: First Responders dispatched by BCEHS who have advised of their intent to use; hospital medical teams; members of the BC Search and Rescue Association (BCSARA) and Canadian Coast Guard and/or Canadian Armed Forces Medical Teams, if trained and used by them.
Currently BCEHS is a partner in the CanROC ECPR (ECMO)33 study for refractory out-of-hospital cardiac arrest with the study protocol including the pre-hospital placement of LUCAS device on the study population. It may be possible depending on evidence from that trial that at a later stage a cohort of BCEHS Specialist Paramedics or Advanced Care Paramedics may join this list of appropriately trained persons.
CONCLUSION
Many studies and meta-analyses have recognised that outcomes with mechanical CPR especially survival to discharge, neurological status and in some cases ROSC alone, do not either match or surpass results where high quality manual CPR is possible and provided. However, it’s clear that mechanical CPR has its place where manual CPR is not possible or difficult, or as a bridge to advanced therapies.
The question though remains why mechanical CPR with its advantages does not perform as well as manual CPR with all its inherent challenges? The fact that one of the biggest trials, CIRC23 of a mechanical CPR device involved a complex statistical analysis to evidence only equivalency adds to the concerns regarding the empirical evidence supporting mechanical CPR.
Evidence suggests that use of mechanical CPR does not lead to improved survival rates and neurological outcomes, but have we truly compared consistent measures in these trials? Wyer27 reminds us that we need to understand patterns of effect. Is there bias in the belief that the use of mechanical CPR leads to worse outcomes because it’s not proven otherwise, or is the reality that the use of mechanical CPR restores cardiac output temporarily for patients that previously would have treatment terminated on scene? Meta-analysis of data relating to in-field discontinuation of resuscitation between mechanical CPR and manual CPR may also inform the discussion around differences in survival rates.
Has statistical analysis truly compensated for confounding variables when looking at survival rates between manual CPR and mechanical CPR? The reality may be that 30- day survival rates are no worse or even better for mechanical CPR than when every cardiac arrest patient was transported to hospital with no in-field discontinuation of resuscitation.
Newberry et al.30. also questions treatment guidelines and protocols used for resuscitation with mechanical CPR devices as they are based on the research and physiological response to manual CPR. LINC25 addressed this with changes to the resuscitation protocol for those patients being treated with the LUCAS device, suggesting that further understanding of the impact of these changes was required.
New evidence may come from clinical trials looking at outcomes for OHCA patients with resuscitation protocols around airway management, pharmacological protocols and discontinuation of resuscitation designed specifically for use with mechanical CPR devices. These may answer the question of why mechanical CPR does not appear to perform as well as manual CPR.
It is obvious that mechanical CPR technology should not be dismissed or ignored for OHCA. The value of mechanical CPR devices in the field to support ongoing hospital therapies is recognised, many post-arrest patients are being transported by air medical transport to centres of care and no doubt there will be improvements in design and training for their use.
LOOKING TO THE FUTURE?
It is said that one should always end on a positive note. A 2009 French34 study took three groups of French Red Cross First aiders (n80) who were unfamiliar with AutoPulse and with minimal awareness (one group had two illustrations, one had four illustrations and the final one had a five minute video and familiarisation time with the device) and asked them to place on a manikin. With this small amount of training the last group (video and handling) were able to place the device with no errors in placement in 19 seconds and the time to first compression was 48 seconds.
In an environment where we coach CPR and guide the use of an AED on the phone, is it unreasonable to expect to see the use of mechanical CPR devices by the general public and for them be as common as AED’s or re extinguishers in buildings once we have the answer to the questions posed here?
REFERENCES
1. 10 Steps for Improving Survival from Sudden Cardiac Arrest, Resuscitation Academy, Seattle: http://www.resuscitationacademy.org/downloads/ebook/TenStepsforImprovingSurvivalFromSudde nCardiacArrest-RA-eBook-PDFFinal-v1_2.pdf
2. PhysioControl LUCAS http://www.lucas-cpr.com/en/lucas_cpr/lucas_cpr
6. Perkins et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised controlled trial. Lancet 2015; 385: 947-55
7. ZOLL AutoPulse Clinical Studies
8. Steinmetz J, et al. Improved survival after an out-of-hospital cardiac arrest using new guidelines. ACTA ANAESTHESIOLOGICA SCANDINAVICA doi: 10.1111/j.1399-6576.2008.01657.x
10. Jennings PA. at al. Ef cacy of AutoPulse compared with standard chest compressions for out- of-hospital resuscitation: A matched case–control study. Resuscitation Vol 81 Issue 2 Supplement Page S20
11. Ong MEH et al. Use of an Automated,
Load-Distributing Band Chest Compression Device for Out-of-Hospital Cardiac
Arrest Resuscitation JAMA, June 14, 2006—Vol 295, No. 22
12. Casner M, et al. The impact of a new CPR assist device on rate of return of
spontaneous circulation in out-of-hospital cardiac arrest. Prehosp Emerg Care.
2005 Jan-Mar:9(1):61-7.
13.
https://eccguidelines.heart.org/index.php/circulation/cpr-ecc-guidelines-2/part-2-evidence-
evaluation-and-management-of-con icts-of-interest/
14. Steen S et al. Evaluation of LUCAS, a new device for automatic mechanical compression
and active decompression resuscitation. Resuscitation 55 (2002) 285-299
15. Rubertsson S, Karlsten R. Increased
cortical cerebral blood ow with LUCAS; a new device for mechanical chest
compression compared to standard external compressions during experimental
cardiopulmonary resuscitation. Resuscitation 65 (2005) 357-363
16. Wang et al. Load-distributing band improves ventilation and hemodynamics
during resuscitation in a porcine model of prolonged cardiac arrest.
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012,
20:59
17. Wik L et al. Quality of Cardiopulmonary Resuscitation during out-of-hospital Cardiac Arrest. JAMA (2005) Vol 293, 299-304 18. Fox J, Fiechter R et al. Mechanical versus manual chest compression CPR under ground ambulance transport conditions. Acute Cardiac Care, 15:1, 1-6
19. Jones AYM, Lee RTW (2005) Cardiopulmonary resuscitation and back injury in ambulance of cers. Int. J Occup Environ Health 78: 332-336
20. Smekal D, Lindgren E, Sandler H, Johanseen J, Rubertsson S. CPR-related injuries after manual or mechanical chest compressions with LUCASTM device: A multicentre study of victims after unsuccessful resuscitation. Resuscitation 85 (2014) 1708-1712
21. Paradis NA et al. Abstract P74: The California AutoPulse Quality Assurance Registry. Circulation 2009; 120:S1457
22. Couper et al. Mechanical devices for chest compression: to use or not to use. Curr Opin Crit Care 2015, 21:188-194
23. Wik et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation 85 (2014) 741-748
24. Buckler DG, Burke RV, Naim MY, MacPherson A, Bradley RN, Abella BS, Rossano JW for the CARES Surveillance Group. Association of Mechanical Cardiopulmonary Resuscitation Device Use With Cardiac Arrest Outcomes. Nov 2016.
25. Rubertsson S et al. Mechanical Chest Compressions and Simultaneous De brillation vs Conventional Cardiopulmonary Resuscitation in Out-Of-Hospital Cardiac Arrest: The LINC Trial. JAMA. 2014; 311(1); 53-61
26. Gates et al. Mechanical chest compression for out of hospital cardiac arrest: Systematic review and meta-analysis. Resuscitation 94 (2015) 91-97
27. Wyer P. Review: Mechanical and Manual CPR do not differ for survival or neurological outcome in out-of-hospital cardiac arrest. Annals of Emergency Medicine ACP Journal Club April 2016
28. Bonnes JL et al. Manual Cardiopulmonary Resuscitation versus CPR Including a Mechanical Chest Compression Device in Out-of-Hospital Cardiac Arrest: A Comprehensive Meta-analysis From Randomized and Observational Studies. Annals of Emergency Medicine 2016 Mar;67(3): 349-360
29. Westfall et al. Mechanical Versus Manual Chest Compressions in Out-of-Hospital Cardiac Arrest: A Meta-Analysis. Crit Care Med. 2013 Jul;41 (7): 1782-1789
30. Newberry R et al. No Bene t in Neurologic Outcomes of Survivors of Out-of-Hospital Cardiac Arrest with Mechanical Compression Device. Prehospital Emergency Care, 2018 May- Jun;22(3):338-344
31. Salcido et al. Incidence and outcomes of rearrest following out-of-hospital cardiac arrest. Resuscitation 2015 Jan;86:19-24
32. Jabbari et al. Incidence and risk factors of ventricular brillation before primary angioplasty in patients with rst ST-elevation myocardial infarction: a nationwide study in Denmark. J Amer Heart Assosc. 2015;4:e001399
33. Extracorporeal Cardio-Pulmonary Resuscitation (ECPR) using Extracorporeal Membrane Oxygenation (ECMO) BC ECPR Trial for Out-of-Hospital Cardiac Arrest NCT02832752
34. Lapostolle et al. Use of an Automated Device for External Chest Compressions by First-aid
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-12 12:29:222019-08-13 11:16:08The use of Mechanical CPR Devices in a pre-hospital setting: A review of the literature with recommendations for clinical utilization
Published in: Autumn 2018 Edition of Ambulance Today Magazine
The value of innovation to patient care cannot be overstated, but its further benefits of efficiency and cost-effectiveness within the NHS make it a vital and ongoing campaign. In this joint article, Professor Andy Newton offers some valuable insights into the value of continued innovation across the NHS before shining some light on clinical simulation in particular. Senior Education Manager at SCAS, Darren Best, then introduces us to the advanced facilities and training going on at their new Education and Enhanced Simulation Centre in Newbury, Berkshire.
Innovation and why patient care needs more of this elixir
Healthcare is no stranger to innovation, and to its credit, the National Health Service has an enviable track record of deploying new methods and technology across a spectrum of patient needs. Examples such as Magnetic Resonance and Computer Tomography, are well known and many others across the spectrum of therapeutics, prosthetics, the application of genetics and more recently robotics continue to capture the imagination of the public and those who work in healthcare alike. South Central Ambulance Service’s new Education and Enhanced Simulation Centre is a forward-thinking example of innovation which applies directly to the field of paramedicine.
The NHS even has an ‘Innovation Accelerator’ programme and a well-promoted list of innovations, including items of direct relevance to those who have an interest in Paramedic and Ambulance matters generally, such as the National Early Warning Score, NEWS. Innovation therefore doesn’t have to be about new products, but can extend to new methods of assessment, new ways of designing, clinical process, where telephone triage could be viewed as a highly relevant example, or in services and new ways of training, about which more in a moment, as well as to many other aspects of care and quality improvement.
But innovation is hard, it is not always welcomed and can often be resisted by those who, for whatever reason, are less attuned to change, not least by those in authority or their confederates who seek the status quo and an easy life free from excitement and risk. It is therefore particularly welcome when innovation works, because it is very likely that the innovation concerned will have been in no small part a function of effective leadership. Leadership that will have come from the hard work, blood, sweat and tears of a few highly energetic individuals who have battled against inertia and the often-lukewarm desire of bureaucratic organisations to modernise. All because the personalities involved have a desire to see services improve for patients and staff alike.
The Innovation of Clinical Simulation
South Central Ambulance Service’s new simulation centre will be judged by the above criteria– the innovation of simulation applies directly to the work of ambulance crews and holds out the promise of raising the quality of patient care. Clinical simulation has a surprisingly long history and demonstrates how several trends have come together to create a series of technologies and teaching methods which, in the right hands, are much more than the sum of their parts. Simulation training represents the vital partnerships that are so necessary between industry and clinicians, with the skills and abilities of both groups demonstrating the very positive results of pooling their talents.
There is no doubt that clinical simulation, when applied to the education of ambulance staff, as with other groups of health care workers, can have a very positive effect on raising competence and greatly helps to prepare for the challenging world of pre-hospital care delivery. This area has also become a much better researched area of practice and while there is insufficient time to do this important aspect justice in this short piece, the evidence base is growing at a rapid rate. It is, however, very important never to over-emphasize the role of the technology over the role of the teaching faculty, the quality of teaching scenarios and the process of debriefing, as well as the reflection of the processes of learning generally. Clinical is therefore one of those innovations that few in the business of clinical education would wish to be without. It is a set of methods that, at its best, integrates sound educational approaches, with a well-designed curriculum and teaching methods, with digital and physical technologies that increase the changes of producing high quality practitioners and that is a goal worthy of the leadership efforts involved.
Andy Newton, 27th August, 2018
The SCAS Education and Enhanced Simulation Centre
In the last three years, South Central Ambulance Service’s Education team has revolutionised the delivery of pre-hospital education and training. The SCAS Education and Enhanced Simulation Centre based in Newbury, Berkshire provides high-technology learning environment facilities that simulate settings ambulance crews would encounter daily. Six purpose- built training and environment rooms allow recreation of the patient’s journey, from their home environment (including a bathroom, kitchen and bedroom) through treatment enroute to hospital in the Mobile Simulated Ambulance (Simbulance) to handing over the patient in the Emergency Department (ED) resuscitation bay. The centre also houses a multi-purpose skills room for delivery of a range of skills from manual handling training for patient transport staff to invasive cannulation and suturing for specialist urgent care paramedic/ practitioners. Collaborative multi-agency working is facilitated in a mock flat which has been used to great effect in joint police and ambulance mental health awareness training.
The pièce de résistance is a fully immersive projection room enabling multi-environment training. This places ambulance staff at a variety of locations such as on a motorway, in a children’s playground or even at a marina!
Education sessions are controlled via a central control room where the simulation technologist can operate all rooms with interactive bespoke software and tablet technology designed specifically for the centre. This allows the creation of safe, realistic scenarios conducive to learning. All training rooms have audio and video capability with playback analysis and feedback available in a dedicated debriefing room on an interactive SMART TV, with the addition of glass whiteboards with street-map view projection for major incident table-top exercise learning.
Simbulance is housed within the centre, and when docked, it can be used as an integrated training area connected to the network and controlled via the central control room. Undocked, Simbulance can be driven to local or cross-border ambulance stations to be used as a standalone simulation facility. This increases the capacity and capability to deliver dedicated training sessions without placing strain on ambulance operational demand.
I am proud to lead the Newbury Education and Simulation training centre alongside a dedicated team of clinical (doctors, paramedics and midwives) and non-clinical educators on the teaching faculty. Together they facilitate a range of sessions from Trust statutory and mandatory education to partnership community maternity and mental health training. The facility has been utilised by all grades of staff including patient transport staff, front-line paramedics and specialist operational teams such as HART. Importantly, the centre also provides a safe space for operational officers to develop and retain clinical and non-technical skills.
The Education and Simulation Centre team has provided pre- hospital training to multi-disciplinary and inter-professional healthcare groups by delivering previously unheard-of immersive capabilities. By promoting and expanding training realism, we have enabled role advancement, staff development and workforce stability, thereby providing safer patient awareness and patient care.
Darren Best, Senior Education Manager, SCAS
To find out more
about South Central Ambulance Service, please visit their website: www.scas.nhs.uk
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-12 11:53:352019-08-13 11:16:26The value of clinical innovation in enhanced ambulance simulation training
The Miscarriage Association has developed a new e-learning resource to support medical professionals in providing the best care they can to women experiencing pregnancy loss.
The resource is based on the real experiences of health professionals and those who have experienced miscarriage, ectopic or molar pregnancy, and includes films and interactive activities.
The resource takes around two hours to complete, and is an excellent tool for continuing professional development and learning towards revalidation.
Ruth Bender Atik, National Director at the Miscarriage Association, said: “Pregnancy loss can be a deeply distressing experience and the support health professionals give can make all the difference to helping women through this difficult time.
“We know it isn’t always easy for those working in clinical environments to find the time to reflect on the care they provide. This is why we wanted to create a resource that they can dip in and out of and access easily from their phone, iPad or computer, so the training is available to them anytime.”
The five units focus on different aspects of care, such as having difficult conversations, considering language, and taking care of your own wellbeing while providing care.
Cerian Gingell has experienced two miscarriages and is passionate about improving the care that is provided to those who experience pregnancy loss.
Cerian, said: “Miscarriage is a devastating loss, often without explanation. Nothing can take the pain away, but a kind word, the correct information on what to expect next, the truth about what’s happening – these things can all help make a horrible experience slightly less horrible.
“To me, good care is saying ‘I’m sorry your baby’s gone, it wasn’t your fault’. It’s letting me cry, answering my questions with honesty and sensitivity, reassuring me that because it’s happened once it doesn’t mean it’ll happen again. It’s about respect, sympathy and honesty.
“I think this resource is so important and will help create more consistent care across the country. Every single person that goes through pregnancy loss deserves to be treated with dignity and compassion. Whether they’re speaking to their GP or being treated in hospital, every contact can have a huge impact on the way that person copes with their loss.”
The resource was peer reviewed and produced with the help of Janet Birrell, Gynaecology Matron at Western Sussex Hospitals NHS Foundation Trust, Dr Nicola Davies, GP at The Pinn Medical Centre, Annmaria Ellard, Miscarriage Specialist Nurse at Liverpool Women’s NHS Foundation Trust, Amanda Mansfield, Consultant Midwife at London Ambulance Service NHS Trust, and the Association of Early Pregnancy Units.
Dr. Sarah Bailey, Lead Nurse Recurrent Miscarriage Care and Clinical Research Specialist at University Hospitals Southampton, said: “The Miscarriage Association’s e-learning resource is extremely useful, informative and easily accessible.
“I would thoroughly recommend this excellent training package to any care professional who is involved in caring for women with miscarriage.”
You can access the e-learning resource at: Bit.ly/2Gtniu9 or call the Miscarriage Association on 01924 200795to find out more.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-09 12:04:492019-08-13 11:14:03The Miscarriage Association launches new e-learning resource for medical professionals
A Newcastle man was effectively dead for 20 minutes, but Bruce Carter is alive thanks to his brother, a passer-by and a team from the North East Ambulance Service.
Bruce, a 61 year-old self-employed plumber, suffered a cardiac arrest while out cycling around Tyneside with his brother Tristram. The brothers were reunited with the ambulance crew so Bruce could thank them.
Tristram takes up the story of what happened on the day.
“We had cycled to North Shields and got the ferry. He said he felt uncomfortable, with pains in his shoulders, but I put that down to the fact that he hadn’t been on a bike for quite some time. We were going to get the Metro back. We were pushing our bikes up a road to Chichester station.
“I was slightly ahead of him but when I looked back he was down on the ground. I was expecting him to be dehydrated and suffering from heat exhaustion but when I got to him he was totally lifeless. I started CPR (cardiopulmonary resuscitation). A passer-by called Peter offered to help, so he took over while I rang for an ambulance.”
Clinical advisor Lisa Ahmed took the call from Tristram. “It was clear he and the passer-by were doing a really good job with CPR. They were very focussed and it was crucial that CPR was administered so quickly.”
The Monkton-based crew of paramedic Michael Hugo, student paramedic Paul Wales and emergency care assistant Emma Newton were only minutes away when they got the call to respond.
Michael said: “Paul took over CPR and we realised he was in ventricular fibrillation which is a cardiac arrest and required a defibrillation shock so his heart could then be re-started. After the shock CPR continued and eventually his heart went into a normal rhythm.
“We got him on to a stretcher and into the ambulance. By the time he woke up, he was understandably very confused and didn’t know where he was. The one thing he did say was that he didn’t want to go to a ‘red and white’ hospital!
“Effectively he had died for 20 minutes – he had stopped breathing and didn’t have a pulse. His brother and the passer-by helped to save Mr Carter’s life – he needed CPR with the initial cardiac arrest.”
Paul said: “Tristram and the passer-by were doing excellent compressions when we arrived.” While for Emma, it was the most dramatic case after changing jobs a couple of months ago from being an office-based health advisor to working on an ambulance.
Mr Carter was taken to South Tyneside Hospital, and then transferred to the Sunderland Royal Hospital where he had stents inserted.
Bruce, from Thorntree Drive in Newcastle, said: “My brother is trained in first aid and used CPR – that’s probably what saved me – meaning my brain wasn’t starved of oxygen.
“I’m very grateful to the crew. They were fantastic, helping to treat me and reassuring me. I just wanted to thank them personally for what they did. At first I was making light of what happened, but after a couple of days the seriousness of what happened struck home.”
Tristram, an RAF Squadron Leader who works in air safety, added: “The ambulance crew were wonderful, they were the ones who brought him round.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-09 11:43:382019-08-13 11:14:12Brother and ambulance crew get Carter – just in time
Jerusalem, July 2nd, 2019 - United Hatzalah volunteer Yisrael Shavit saved a young girl in Hadera from choking on Sunday evening. After arriving in less than a minute at the scene of the incident, Shavit managed to single-handedly treat and rescue an infant from what could have been her death.
Shavit described the dramatic story. “I was davening Mincha at Shul and I received an alert on my bluebird radio from dispatch. The alert said that a young toddler, about six-months-old was choking right near my location. I raced to my ambucycle and jumped on and rushed to the address. I saw a group of people standing around two parents who were holding their child in front of them. The father was slapping an infant girl on the back. I asked to take the child. She was making choking noises which meant that her airway was partially blocked. She had started to turn blue.
I looked inside her mouth and saw a small edge of what looked to be a bit of plastic stuck in her trachea. When I slapped her back, a bit more popped up. I stuck my finger in her mouth and after a few tries, was able to grab hold of and remove the plastic. It was a wrapper from an ice pop. Once the blockage was removed the child once again began crying.
The girl’s parents were so thankful for my quick arrival and successful assistance that they kissed me on the forehead in the middle of the street just as other EMS volunteers began arriving.
It was a few minutes before the ambulance came, they had a very healthy and stable patient who was taken to the hospital for follow-up care.
I’ve been at choking calls before but usually, you arrive after the person has choked and you need to do CPR. This is the first time I was able to arrive while it was still happening. I am happy that I was able to help and that I was a messenger of salvation in this instance. This is why I joined United Hatzalah. It is the reason the organization exists and why all of the volunteers do what we do.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-09 11:36:152019-08-13 11:14:49Interrupting Prayers To Save A Choking Infant
Jerusalem, June 12th, 2019 - United Hatzalah volunteer EMT Noa Salant was shocked when she responded to an emergency incident to find her mother to be the patient in need of medical care.
The family was supposed to get together for some quality time and both Noa and her mother were arriving by bicycle from different locations. “As I was driving, I heard screams from up ahead of me and saw a few people standing around someone lying on the street,” said Salant sometime after the incident which occurred two weeks ago.
When Salant arrived at the scene she saw a very familiar woman lying on the sidewalk injured- her mother. “I immediately went into EMT mode and began triaging her. I took her pulse while simultaneously calling for an ambulance. I asked the people around her if anyone saw what happened and all they would share was that she fell.”
Noa (right) and her mother.
Salant relived the dramatic moments of the treatment. “I noticed that my mother could not move her pelvis. I began treating her for her injuries and immobilizing her so that none of the injuries would get worse. Other volunteers from United Hatzalah began arriving and they assisted me in providing treatment. When the ambulance came some ten minutes later, I joined the team on the ambulance and kept watch over my mother the entire way to the hospital. When we arrived at the emergency room we found out that she had broken her hip.”
Salant spent the next few days visiting and caring for her mother in the hospital. “The doctors told us that this is the type of injury where there is no corrective surgery and that the best medicine is to keep my mother stable and her spirits up in order to give her body time to heal. They added that the care I gave at the scene prevented the injury from getting worse. It is thanks to the training that I received from United Hatzalah that I was able to keep my cool and follow all the procedures and protocols necessary even though I was treating my own mother,” Salant concluded.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-09 11:30:202019-08-13 11:15:22Treating My Own Mother
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, you cannot refuse them without impacting how our site functions. You can block or delete them by changing your browser settings and force blocking all cookies on this website.
Google Analytics Cookies
These cookies collect information that is used either in aggregate form to help us understand how our website is being used or how effective our marketing campaigns are, or to help us customize our website and application for you in order to enhance your experience.
If you do not want that we track your visist to our site you can disable tracking in your browser here:
Other external services
We also use different external services like Google Webfonts, Google Maps and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.